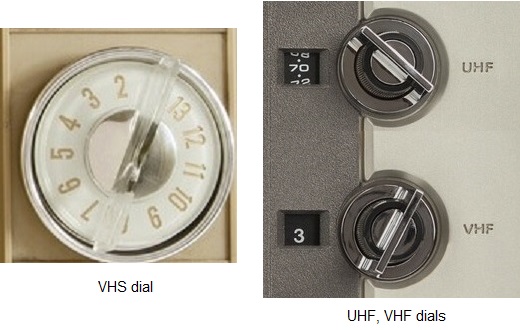
We lived in Bisbee, Arizona from the late 1950s until the mid-1960s. The nearest television stations were 100 miles away in Tucson, far beyond the range of “rabbit ears” antennas, so rural communities like ours had Community Antenna Television (CATV). Several towers erected on Juniper Flats, a plateau on the mountain northwest of town, captured VHF (Very High Frequency) signals and distributed them to houses through coaxial cable. A small adapter allowed one to connect the cable to the two antenna terminals on the back of the TV and voilà! A great picture, no snow, no ghosts and no need to fiddle with a UHF ring tuner (that “U” on the dial). Everyone watched the same shows, and we liked it, dammit!
Rabbit ears antenna
By 1970 cable had became more popular as many households ditched their antennas. The shift happened despite early FCC meddling and intimidating ads the networks aired in movie theaters decrying the evils of “pay TV.” Yet Home Box Office successfully launched in 1972 and has been with us for fifty years.
Televisions changed over the next several years. Manufacturers added a separate UHF dial as more channels became available, eventually replacing both dials with a single internal tuner. Cable connected directly to a coaxial port. Small children served as early channel changers, performing double duty as antenna adjusters. Actual remote controls evolved from wired (Zenith’s “Lazy Bones”) through primitive wireless (Zenith’s “Space Command” and Magnavox’s “pig whistle”) to ultrasonic and finally infrared.
Videotape became popular in the 1980s but with only one port available, the cable had to be routed through the player/recorder and then to the television. One tuned to Channel 3 or Channel 4 to watch a videotape. Later televisions had two coaxial ports and early game systems supplied a box switch.
An alphabet soup of basic cable networks – CNN, TBS, TNT, CBC, TLC, VH1 and others – proliferated during the 1980s. A smarmy meme noting MTV’s 40th anniversary read, “Thanks for 12 years of great music!” Basic cable provided us with “hundreds of channels and nothing worth watching,” but the cable companies hadn’t yet evolved into the rapacious apex predators we loathe.
Then the Internet happened.
Those of us who bought the first home computers remember primitive online communication through dial-up Internet Service Providers (ISP) like Prodigy, Compuserve and, of course, America Online (AOL). Who can forget the gentle sounds of your computer modem trying to connect with the AOL servers? A 14,400 baud modem gave me the blinding transmission speed of 14.4kbps to go along with my 16mHz computer clock speed. Those were the days!
But dial-up tied up one’s landline and few people could afford to spring for a second line. It was also expensive; AOL charged an hourly fee until it switched to a flat monthly rate. My 14-year old son ran up a $400 AOL bill during August 1996. (Boy, you gonna be mowing lawns until your 20s!)
Cable companies saw an opportunity and would soon pounce.
Bombastic Cable Pirates provided our cable when we moved into our house in 1998. Our Internet was still a DSL (Digital Subscriber Line) shared with a fax line. I don’t remember how much it cost, but it seemed reasonable at the time. That is, until the price jumped after the two-year introductory rate ran out. Peg was able to talk them into continuing the lower rate a couple of times, but that didn’t last. Most cable providers enjoy near-monopoly status and are only interested in hooking new customers, not retaining their existing ones.
Or, to quote Leo Getz: “They fuck you! They fuck you! They fuck you! “
We didn’t mind the price increases until they started eliminating channels, one by one, from our tier, moving them into the higher tier which cost a lot more. Complaining fell on deaf ears, as Stan and Kyle discovered when they confronted their local cable company. So, when Awesomely Terrific and Tremendous showed up in our neighborhood, promising much better customer service AND broadband Internet, we jumped – from the frying pan into the fire.
We signed up for the company’s Triple Delight package: cable, broadband internet, and switching our landline to VOIP (Voice Over Internet Protocol). The Triple Delight with Eggroll Cellular Service would have given us an additional discount, but a few years back, Awesomely offered me $600 to leave while I was working a long-term job in Nebraska. They’d assumed I’d moved there and were not pleased having to pay service fees for another company’s network every time I used my phone, even though my billing address was still in Illinois.
We were content with them for the next several years, until the inevitable price hikes started. Again, Peg managed to bargain for a lower rate a few times, but then our Internet started dropping out, first occasionally, then daily, then multiple times a day, making it completely unreliable. The modem frequently reset itself at odd times, or we had to manually reboot the system, watching that little grey circle go round and round, sometimes for several minutes. Calling Awesomely Terrific and Tremendous to complain went nowhere. “Bob” or “Dylan” or “Steve,” tech support guys with thick South Asian accents, would “run diagnostics” or fiddle with something remotely, promising resolution which never materialized.
Eventually we contacted Bombastic, which had been renamed Sempiternity (“We’re everywhere; there’s no escape!”) in January 2021. They said, “We’ll be happy to come out but you have to clear a path in the snow so we can get to the box.” Would you also like hot cocoa and cookies? They wouldn’t be able to bury the new cable until the ground thawed, so we opted to wait until fall.
A Sempiternity technician installed the new system in early November. It took him two hours to decipher the previous wiring, but he was very pleasant and thorough. He told us we might need to get one of Sempiternity’s new Wi-Fi capsules to boost our upstairs signal.
The only glitch was the need to exchange the upstairs cable box, which inexplicably turned itself off and on every ten minutes. I exchanged it at the local Sempiternity store relatively quickly and we were in business. (I had to ensure the lawn service people didn’t run over the exposed cable during their last visit of the season, but we had a relatively warm late fall, and they buried the cable before Christmas.)
When we were sure everything was working, Peg called Awesomely Terrific and Tremendous to cancel our subscription.
“We can’t cancel it today because our network is down.” Ah, the irony.
Even more ironic was the Saturday Night Live skit, airing two days later, about one man’s ordeal trying to cancel his cable subscription.
All was going well until I bought the Wi-Fi capsule. But that’s a story for the next post
(I took a few months off because I didn’t have much to say. and I wanted the tangible rewards of “döstädning” (Swedish death cleaning). We emptied the storeroom Peg rented for her parents‘ things after her father’s passing. The memorabilia and the coming New Year’s Eve folderal prompted this memorial.)
Many people make resolutions on New Year’s Eve, most of which won’t last the month. But this one lasted a lifetime.
Mike was born in Chicago in 1919 to James and Anna Sullivan, immigrants from Ireland and Yugoslavia, respectively. They lived on the West Side of Chicago where the Irish and Italian neighborhoods met. His father worked for the railroads and his mother was a housewife; back then married women didn’t aspire to anything else. His little brother Johnny was born a few years later. Mike and his family emerged from the Great Depression intact but, like many from that time, he saved every little thing because, “you never know when you might need it.”
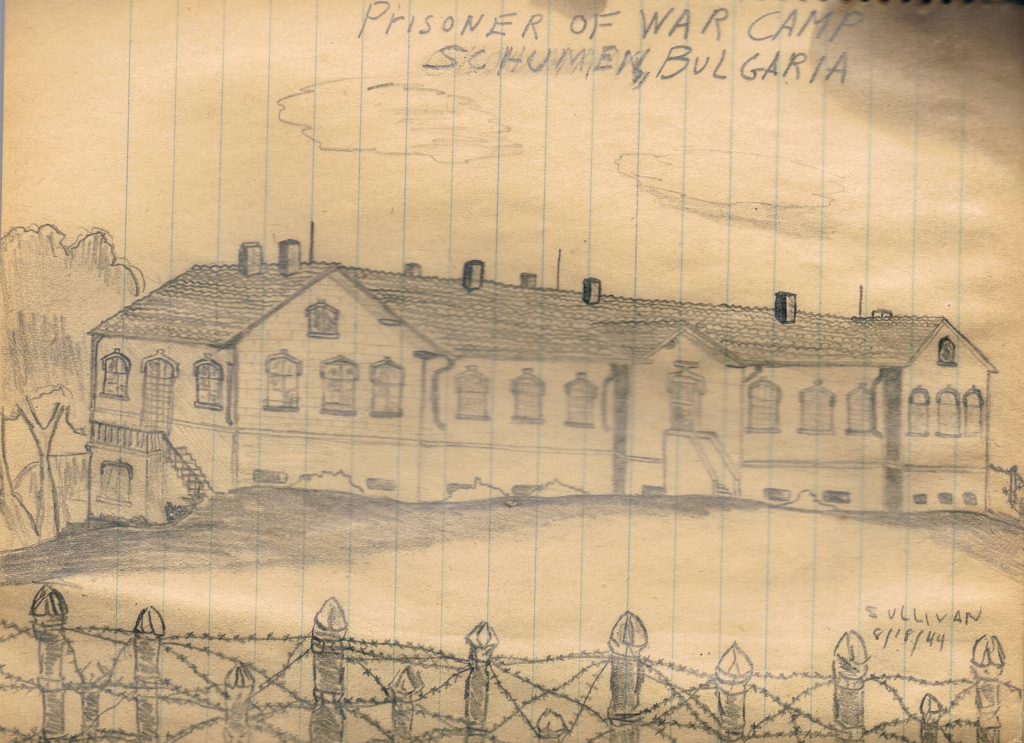
Mike enlisted in the Army when World War II started, earned a sharpshooter rating during sniper training, before becoming a tail gunner in a B-17 Flying Fortress. His plane, the Opissonya, was mortally wounded during Operation Tidal Wave, a raid on the Ploesti oil fields in Romania. Mike was badly wounded and his parachute was riddled with bullet holes. The bombardier, David Kingsley, strapped Mike in his own parachute, tossed him out the door and went down with the ship. He was captured and sent to a Bulgarian prison camp, returning home with memories and secrets he would only share with fellow veterans. When his wife pressed him for details many years later, he would say, “Honey, you don’t want to know. It’s not something I want to remember.”
Sketch from Mike’s diary done while in the POW camp
After the war Mike returned to Chicago and moved back to his parents’ house. A budding artist, he enrolled at the Art Institute of Chicago and then landed a job as a graphic artist. On Saturdays, he and his buddies would go to one of the many dance halls around Chicago for a night of revelry. Sometimes they would crash Italian wedding receptions because there was always great Italian beef and no shortage of gorgeous young women who loved to dance. The revelry would often last until the wee hours of Sunday morning, when they attended the sunrise. Mass before hitting the sack. He was a confirmed bachelor with absolutely no interest in settling down and raising kids. Or so he believed.
Gloria was born on the South Side of Chicago 1933, to Joseph and Nadezda Shiplov, the last of eight children. They emigrated to the United States from “the old country,” although which “old country” was always a mystery. They might have come from Yellow Russia (now Belarus), or maybe Russia proper before it became the Union of Soviet Socialist Republics. Family members were always evasive about their history and any information pried from reluctant lips was suspect. There’s an old picture of Grandpa Joseph in a Cossack uniform, prompting speculation he may have fled the Bolsheviks. He arrived at Ellis Island with, according to his travel papers, a woman who was NOT Nadezda and whose fate remains unknown.
The only person who knew everyone’s secrets was old Muzyka, the undertaker for the Eastern European community, and he took those secrets to his grave. Peg says, “The Shiplov family crest should be engraved with “??? ???? – Everyone lies!”
Nadezda died when Gloria was two years old, and Joseph was ill-equipped to care for a tosed around among the siblings’ families until her sister Ann, twenty years her senior, and her husband John took Gloria in and raised her as their own.
Ann Morgan and Gloria Shiplov, age 6
Gloria graduated from Jones Commercial High School, a prestigious and rigorous institution that provided students a well-rounded education with business and personal training highly sought by employers. She learned secretarial skills and bookkeeping, but she dreamed of becoming a nurse. She was lucky enough to get a full scholarship to nursing school, on the condition that her family provide a small monthly sum for “incidentals.” Her father refused and never offered an explanation, so Gloria found a secretarial job at Teepak, a company that manufactured meat casings. Maybe his decision was rooted in Russian pride, or maybe he believed a woman should never aspire to be more than a housewife and mother. I’d like to think it was divine intervention, a little nudge in the direction of the inevitable.
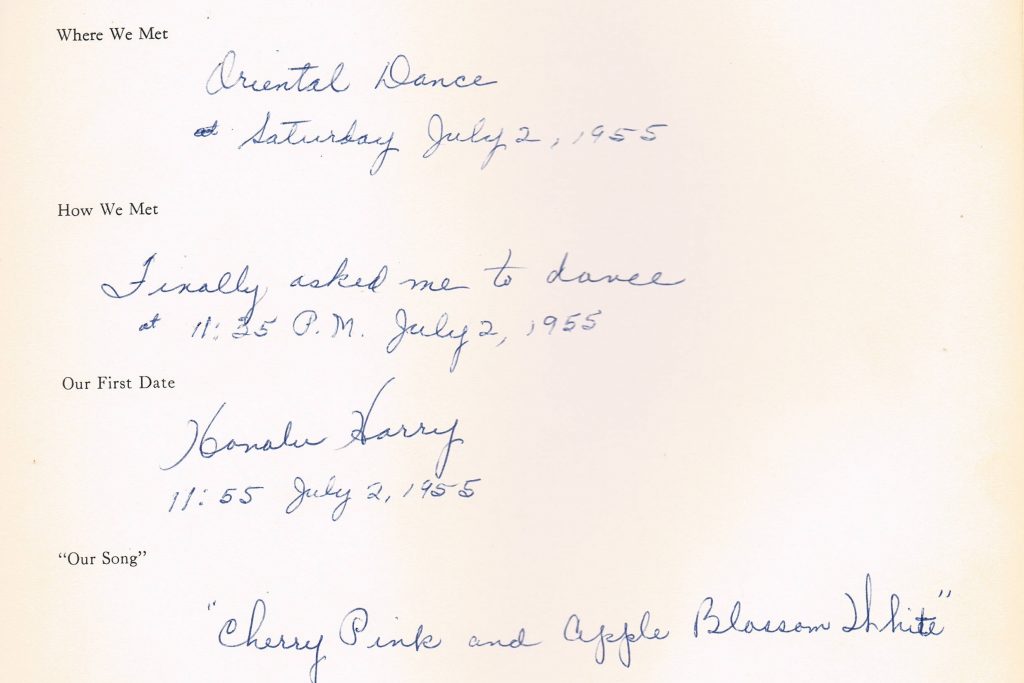
On Saturday nights Gloria and her pack of girlfriends made the rounds, dancing with eager young men at the dance halls or sometimes with soldiers at the local USO. One sultry summer evening in July she and her best friend, Marge, went to a “28-and-older” dance, even though Gloria was only 22 at the time. Mike Sullivan was also at that dance, and at the time had been dating three or four women, including one who assumed they were engaged, although no such proposal had ever been offered. He was still footloose and fancy free, committed to remaining single.
That changed at 11:35pm.
Gloria may have noticed him first because she later wrote “Finally asked me to dance at 11:35pm July 2, 1955” in her bridal keepsake book. Twenty minutes later they went to Honolulu Harry’s Waikiki for their first date. That was a much different time as few women today would leave with a man she’d only known for 20 minutes. But the heart knows what it wants. Later he would tell his daughters “I knew she was the one.”
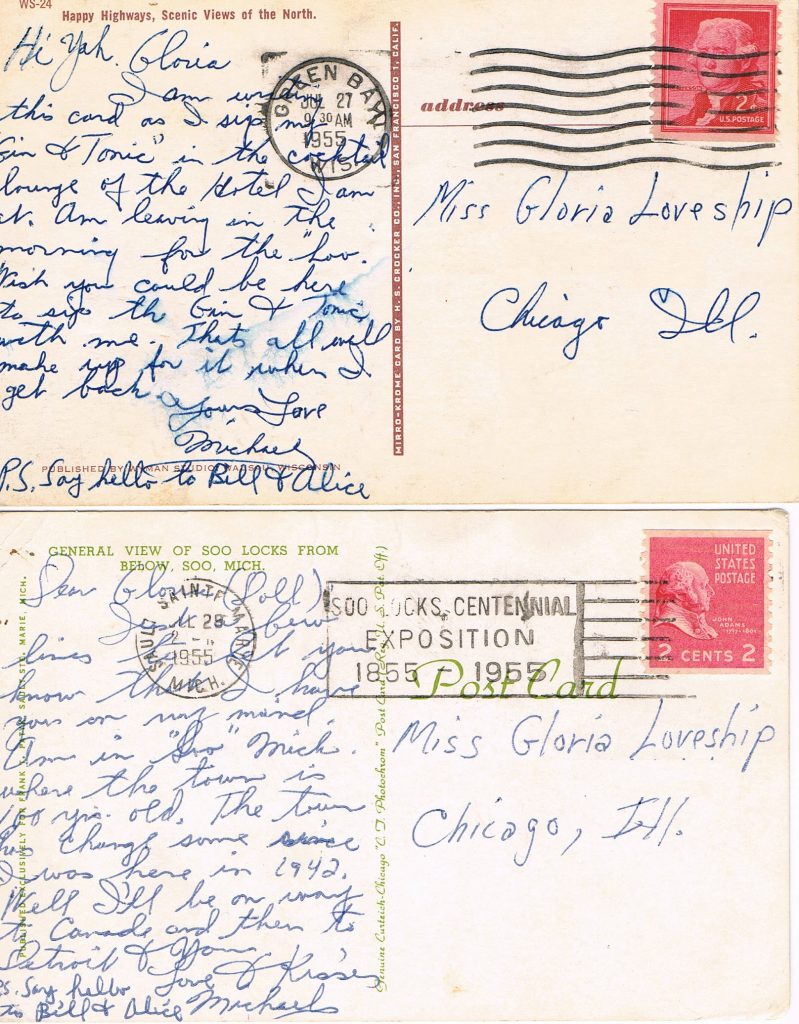
A few weeks later Mike was in Sault Ste Marie, Michigan, on his way to Canada and then Detroit to visit family. Never one to worry about minor details, he sent several postcards to Gloria “Loveship.” He lamented she was not with him in the hotel lounge to “sip the gin and tonic with me” and vowed to make up for the separation upon his return.
Gloria and Mike were inseparable. They celebrated Mike’s birthday at their favorite restaurant, Honolulu Harry’s that fall and her birthday a few months later.
New Year’s Eve 1955 was very special. They were gathered at the home of her sister and brother-in-law, Alice and Bill, to see in the New Year. At 7:40pm, Mike took Gloria’s hand into his, slipped a ring on her finger and said, “You’ll get the mate in six months.” When asked decades later why he didn’t formally say, “Gloria, will you marry me,” he replied, “There wasn’t any need because I knew she’d say ‘Yes!’.” In June 1956, she “got the mate.”
Gloria and Mike’s wedding
Mike, the formerly confirmed bachelor, settled down with the love of his life. They had two daughters and moved to the suburbs in 1964. He worked as a commercial artist at several companies in downtown Chicago until retiring in 1989. He turned down any promotions that would have meant less time with his family. He became notorious for “train-skunking” – scavenging the METRA commuter cars for newspapers and things left behind – a habit which once netted him a new bottle of scotch. Gloria was a stay at home mom until the girls were in middle school; then she worked as an office manager and bookkeeper until she retired.
They had a special ritual they followed every New Year’s Eve. Gloria would remove her rings that morning and Mike would hold on to them. Later that evening during whatever gathering they attended, Mike would have a Manhattan and Gloria would have a martini. At 7:40pm, he would quietly take her hand, slip the rings back on her finger and ask her to marry him. It was a private moment upon which the family would never intrude. They did that for 47 years until Mike’s passing in 2003.
Sometimes there really is a “happily, ever after.”
I worked the midnight shift as an orderly at the local hospital during the summer of 1971, often stayed up late or all night when I wasn’t working so I could maintain the same biorhythm. Sometimes I’d listen to the radio, which in the mid-1960s, fed us a steady diet of three-minute paeans to love, life and the pursuit of the fairer sex. The main sources of pop music in our central Illinois town were Chicago AM stations WLS and WCFL. WLS was the favorite with a host of memorable jocks: Art Roberts, John Records Landecker, Dick Biondi, Clark Weber and the irascible Larry “Uncle Lar’” Lujack.
Pop music started to change during the late 1960s to heavier stuff like Led Zeppelin, Rolling Stones, Crosby, Stills and Nash, Steppenwolf, The Hollies, The Kinks and The Who. Two of The Turtles joined Frank Zappa and the Mothers for a raunchy concert at the Fillmore East. Even the Four Lads from Liverpool had gone to the dark side of drugs, mystical music, and infighting. John Lennon took a lot of shit for claiming the Beatles were more popular than Jesus Christ. We scoured the White Album’s inserts for clues to Paul McCartney’s “death.”
A few of my friends and I were the “goddam hippie-freaks,” as if small-town America had hippies in the early 1970s. High school dress codes banned long hair and beards. Girls still had to wear skirts, even during a -20° windchill winter. There was no heavy drug use (at least of which I was aware). One of our classmates was found sitting up in a sleeping bag in a garage, dead after sniffing airplane glue. Don tried putting peyote buttons in a Dairy Queen strawberry milkshake only to promptly puke it up. Herb bought a test tube of marijuana – mostly stems and seeds – which we stared at intently while huddled in the back of his dad’s Econoline van. I imagined the police would bust in on us at any moment and we’d spend the rest of our lives doing hard time in Stateville among murderers and thieves.
Our band of gypsies gravitated towards less conventional groups, the stuff one would never hear on Top 40 radio: Pink Floyd, Emerson Lake and Palmer, Quicksilver Messenger Service, Peter Green’s Fleetwood Mac, Santana, Traffic, The Band, Grateful Dead and Hendrix. While our classmates listened to The Who’s Tommy, we were splitting our eardrums listening to Live at Leeds, Hendrix’s Electric Ladyland, and Roger Waters’ piercing scream in “Careful With That Axe, Eugene” from Ummagumma. In 1969, Jefferson Airplane’s rebellious Volunteers was the first rock album to get “motherfucker” past the censors (although the OCR of Hair beat them by two years).
A year later, Paul Kantner released Blows Against the Empire, with collaborators Jerry Garcia, Mickey Hart, David Crosby, Graham Nash, and others. The album was a counter-culture fantasy about hijacking a star ship and leaving the earth for utopian pastures, getting a Hugo Award nomination.
One night, while fiddling with the tuner on my compact stereo, I stumbled across a world of music, largely foreign to small-town Midwestern ears, on a radio station out of Little Rock, Arkansas.
KAAY 1090AM is a 50,000-watt radio station in Little Rock, Arkansas. I could only pick up after 10 pm when all the smaller stations shut down for the night. Hearing it for the first time reminded me of when I discovered Radio Havana in 1967 on a leather-clad shortwave transistor radio my grandfather had given me. (Ironically, KAAY also reached Cuba, subverting the “ideological purity” of a generation of Cuban youth. Fast forward 50 years and the Stones play in Havana.)
From 10pm until 2am Clyde Clifford (real name: Dale Seidenschwarz), a laid-back guy with a smooth baritone voice, hosted Beaker Street on “The Mighty Ten Ninety.” It was four hours of “underground” music: much longer tracks; complex musical structures instead of the three-chord formula of pop music; and sometimes controversial subjects. The show’s intro – click here– used a segment of Jimi Hendrix’s If Six Was Nine. Later the intro used a snippet of “House of the Rising Sun” done on a MOOG synthesizer.
Beaker Theater followed at 2 am, broadcasting old radio plays. The only one I remember was a dramatization of Isaac Asimov’s “Nightfall,” a short story about a civilization on a planet with six suns goes mad when an eclipse that occurs once every 2000 years brings total darkness, something they’ve never experienced. (Click here to listen.)
The KAAY managers were too cheap to pay both a DJ and an engineer, so Clyde did both, broadcasting Beaker Street from the station’s transmitter site in Wrightsville, AR instead of the studio in downtown Little Rock. Between song tracks Clyde played ethereal background “music” from “Cannabis Sativa,” by Head, to cover the transmitter’s sounds. Occasionally it ran for several minutes, leading me to believe Clyde had either nodded off or was taking a bathroom break.
Beaker Street introduced me to obscure groups and albums. Spooky Tooth. The Flock. Hawkwind. Bloodrock. King Crimson. Black Oak Arkansas. Black Sabbath, long before Ozzy became an addled old man yelling “Sharon!” Sometimes I’d tape parts of the show with my cassette recorder. The nature of analog tuners meant the signal would periodically drift in and out, interrupting the track, but that was part of the charm when I listened to the tapes years later.
One of my favorites is Jamie Brockett’s “Legend of the USS Titanic.” It’s a completely bizarre fictional account combining historical fact (Jack Johnson, was a turn-of-the-century black boxer), blatant inaccuracies (there was no U.S.S. Titanic), racial stereotypes (“Jews from Miami trading wives and Cadillacs and diamonds”), and modern drug culture (a dope-smoking first mate who carries around “four hundred ninety-seven and a half feet of rope”). The track, running a then unheard-of 13½ minutes, explains the ship sank after the captain, stoned out of his mind, went mano a mano with the iceberg.
Many people remember Welsh guitarist Dave Edumuds for his 1971 AM hit “I Hear You Knockin’.” I remember him for Love Sculpture’s album Forms and Feelings. A heavy metal version of “Mars,” from Gustav Holst’s orchestral suite The Planets, segues into an “amphetamine-fueled rave-up” of Khachaturian’s “Sabre Dance,” which concludes with the last few bars from The William Tell Overture. (“Mars” wasn’t on the original U.K. Parlophone release of Forms and Feelings due to a dispute with the Holst estate, but was included in the U.S. Parrot release.) I kicked myself for not buying the album when I first saw it in the early 1970s before it went out of print. I spent the next four decades years looking for either an LP or CD version, finally acquiring the latter in 2008.
But one song was totally unlike most of what aired on Beaker Street. Late one night I heard “White Bird”, a haunting song by an obscure group with the unlikely name It’s A Beautiful Day. It was exquisite; I would think about it when I stared out of an empty hospital room window during my 2 am break. I began a frantic search for the album, eventually finding it at Arlan’s discount store in Peru, IL, about 30 miles from home.
Clyde left Beaker Street in 1972; the program continued with other personalities until it was taken off the air in 1985. The show was resurrected in 1995 on various Arkansas FM stations before taking another bow in 2011.
Now die-hard fans congregate on the Beaker Street / Clyde Clifford Fans Facebook page, reminiscing about the music that defined us and decrying what passes for contemporary music now. One can now listen to Beaker Street on Friday nights at 9pm Central on the Arkansas Rocks Radio Network.
Some would argue our music was better than what came before and after, but that would be missing the point. Every generation continues the tradition of adding onto that invisible road, paved with infinite combinations of just twelve notes, stretching back millennia. Our music was just a scenic turnout along the way.
Favorite Albums From High School Jimi Hendrix – Electric Ladyland The Who – Live at Leeds Paul Kantner – Blows Against the Empire Quicksilver Messenger Service – Happy Trails and Just for Love Derek and the Dominos – Layla and Other Assorted Love Songs Rolling Stones – Let It Bleed Pink Floyd – Ummagumma The Band – Music from Big Pink Jefferson Airplane – Volunteers The Doors – Weird Scenes Inside the Gold Mine (2-LP compilation)
It started out as a repeat of Wednesday. A lab tech drew blood around 5am which turned out to be yet another set of troponin ($254.00) and lipase ($197.00) levels and a third comprehensive metabolic panel ($202.00) and CBC ($92.00) plus $37 just for the honor of sticking a needle into my veins.
Meghan arrived at 6am to give me my daily Protonix® for reflux; Katrina would bring me the rest of the medications after shift change. This time I balked at the Lovenox.
“Do I really need that? I’ve been out of bed several times and I move around when I’m in bed, so I’m not really going to throw a clot.” “Ok, well, you don’t have to take it if you don’t want it. I’ll let the doctor know.” “While you’re at it, how about asking him to get rid of the telemetry monitor since we know I didn’t have a heart attack and this thing is probably costing someone a lot of money.”
Telemetry was $122.00 per hour and the total charge was $2,074.00 with another $2652.00 “room charge” tacked on.
Then the Parade of the Grey Coats started.
I don’t remember much of what the hospitalist said, aside that my lipase level was back to normal, and he would be talking with the surgeon about our conversation. Peg arrived shortly after he left.
I’m really not sure why the gastroenterologist showed up because he had nothing useful to say. Probably it’s because he could bill $366.30 for the initial consult and $192.03 for the follow up visit. He told me to make a follow-up appointment with him in four weeks, advice I promptly ignored because I’d already made an appointment with my own gastroenterologist to arrange another colonoscopy.
My cardiologist, Dr. McGuinness, recognized me immediately when he arrived. He is also my sister-in-law’s cardiologist, in the same group as her “electrician,” and he is beloved by staff and patients. He should give seminars on bedside manner and patient communication.
“It’s good to see you. I wanted to let you know your stress test was negative. I heard you might be having your gallbladder out soon.” “Yes, I talked with Dr. DeBouw last night; he should be coming around this morning so we can finalize a plan.” “There’s nothing more for us to do, so we’re signing off. I hope surgery goes well.” “Thanks. It was good to see you.”
Peg was in a good mood. However, Katrina, who must have sensed a critically low level of turmoil, arrived to top off the tank.
“Dr. Warner, the hospitalist, said he talked to Dr. DeBouw who said he would talk to you downstairs in pre-op before surgery.”
Peg and I looked at each other.
“Where did you leave it last night?” “He was going to talk to me this morning about doing surgery now or schedule it for a couple of weeks later as an outpatient.” “He didn’t say ‘We’re going to take you to surgery tomorrow,’ did he?” “Nope.” “Well, I hope he’s better in person because right now I’m not happy.”
If momma ain’t happy, ain’t nobody happy!
This could have been problematic. Insurance companies don’t like to pay inpatient rates for outpatient procedures unless done as an emergency, in which case one has to have been formally admitted. Peg had called the claims department on Wednesday and, as of 3:40pm, they had only received notification of my emergency room visit. They weren’t aware that I’d been held for observation, nor whether I’d been admitted. The person in claims said, “Some hospitals are better than others.”
Peg asked Katrina: “Who can I talk to about this? Utilization management?” “That would be a good place to start; you can call the operator and they’ll connect you. You can also talk to the unit manager. I think she is on the floor today.”
Hospital Utilization Management (UM) departments are the bane of every physician’s existence. Utilization reviews ostensibly increase efficiency in hospital care and decreases revenue loss from unreimbursed charges by reviewing care for “medical necessity” and decreasing “length of stay.” Physicians see UM as people paid to tell us what we’re doing wrong and why we should toss patients out “quicker and sicker.”
Peg called UM and got voicemail, which didn’t improve her mood. I called Katrina back into the room.
“Would you do a couple of things for me? First, have someone get ahold of Dr. DeBouw and let him know we want to see him here in the room, not in pre-op. I don’t know if there’s been a problem with communication, but I think it’s tacky to assume someone has agreed to surgery without a final discussion. Then can you find the unit manager because trying to talk with someone in Utilization Management was a bust.”
I sensed some annoyance, but she agreed to contact him. A few minutes later she returned and told us he was on his way to the hospital and would see us before his first surgery. I hated to be demanding, but this is why physicians and nurses need to be on the other side of the bed. It gives the perspective one wouldn’t get without being subjected to the indignities inflicted on the great unwashed.
Dr. DeBouw arrived about 30 minutes later. He reiterated what we had talked about the prior evening, including the risks of becoming seriously ill while waiting to do surgery as an outpatient. Peg was happy again.
Someone from patient transportation came to fetch us around 12:30pm and took us to pre-op holding where patients are prepped for surgery. If you’re lucky, you’ll be put into a 10×12 ft. cubicle with a sliding glass door and a privacy curtain. There’s enough room for the gurney, a small wall-mounted desk and cabinet, an I.V. pump and one family member sitting in an uncomfortable plastic chair. The back wall usually has a fluorescent light bar, a wall-mounted monitor screen, and a “medical headwall system” which has outlets for oxygen, “medical air” suction and electricity. Often there’s a self-inflating resuscitation bag and mask hanging on the wall just in case someone codes in the room. Otherwise, you’ll likely be in a ward with several patient areas separated by curtains, which is also how most Post Anesthesia Care Units (PACU) are set up.
A lively nurse peeked around the curtain and said, “Your doctor will come and talk to you before we take you back.” “Uh, we talked with him upstairs about thirty minutes ago.” Geez, doesn’t ANYONE communicate around here? “Ok then, that makes it easier. What’s your name and date of birth? And what are you having done?”
If I’d thought more quickly, I might have made some smartass comment about having a Cesarean section for twins, but I was really tired and just wanted to get on with it.
The anesthesiologist followed. Anesthesiologists range from gregarious back-slappers through personable, reassuring people to grumpy assholes who speak in grunts. The stereotype of anesthesiologists are physicians who, much like emergency room physicians, prefer short-term, intense patient relationships, minus the need for engaging or conversing.
“What’s your name and date of birth? And what are you having done?” He wouldn’t be the last person to ask me that.
After identifying my name, my quest and my favorite color, I told him about my paradoxical reaction to Versed (midazolam), a benzodiazepine used for sedation for procedures, such as colonoscopies or minor surgeries that don’t require general anesthesia. I’ve been given it for two colonoscopies and my eyelid surgery; apparently, I tried climbing off the table for the first two and a nurse had to hold my head for the third. I don’t remember any of this because Versed puts one in a little black room without anything to distract, like elevator music.
“They gave me 6mg when I had my eyelid done.” (The usual dose is 2mg.) “What??? That was wrong! If the usual dose doesn’t work, giving someone more certainly isn’t going to help.” “Well, they ended up giving me propofol.”
He made a note in my chart and left. A few minutes later the Certified Registered Nurse Anesthetist (CNRA) came into the room. For the uninitiated, a CRNA is a registered nurse who has gone beyond a Bachelor of Science in Nursing (BSN), earning a Master of Science in Nursing (MSN) and completing two to three years of anesthesia training. They’re often supervised by anesthesiologists in large hospitals, but often practice independently in smaller, rural hospitals. They are cheaper to train than physicians and their salaries, while substantial, are much lower than anesthesiologist salaries. I like CNRAs because I don’t have to deal with an outsized ego. With few exceptions I’ve found them to be a joy to work with.
Then the moment of truth arrived. I kissed Peg as they wheeled me out the door and down the hallway. Then down another hallway. And another. By now we should have reached the next county. Finally, they pushed the gurney into the room, and I climbed onto the operating table. The anesthesiologist put a mask over my face and told me to breathe deeply.
I heard, “How are you doing?” “I’m still here.” Not for long, sweetheart.
I’m thoroughly fascinated by general anesthesia. You’re out like a light and before you know it, you’re in the PACU babbling like an idiot. My prostate surgery took three and a half hours, but it felt like ten minutes to me. This was no different. When I woke up in recovery, I asked myself am I dreaming? I’ve had fairly vivid dreams that are almost indistinguishable from real life until I finally wake up. I asked “am I dreaming” out loud but there was still no answer. Slowly things started to come into focus, and I suspected I wasn’t in the OR.
I saw a recovery room nurse next to the gurney, making notes in the laptop sitting on the bedside table. I put my hand on her shoulder to make sure she was real. She took my hand away and looked at me.
“You’re in recovery. Do you need anything?” “How about a beer?” “No, there’s no beer” “I want a beer.” “Nope, no beer.” Well, THAT sucks!
I became aware of a rhythmic beeping sound above my head and to the left, the pitch of which began to slowly decline.
“Take a deep breath.”
I did and the pitch rose. I nodded off and the pitch dropped.
“You have to breathe. Take a deep breath”
The beeping sound was coming from the pulse oximeter, a device which measures the percentage of blood oxygenation saturation (also known as O2 sats) through a small sensor clipped to one’s index finger. Anything above 98% in a healthy person is normal. I’ve had lifelong asthma and chronic inflammation, so my sats run around 95% on a good day.
I looked over my shoulder; my O2 sat was 89% and going down. I took a few deep breaths and it rose to 98%. Every time I heard the pitch going down, I looked at the oximeter and adjusted my breathing because I don’t like being yelled at even though I know I’m just fine. I’m not breathing deeply because I just had three tent stakes thrust through my abdominal wall and I was breathing anesthetic gas, which I could still taste an hour later.
“Would you like some ice chips?” “Yes, please.”
She dumped a spoonful of ice chips into my mouth which I savored, waiting for them to melt instead of chewing.
“Can I have more ice?”
Another spoonful of cool, wet ice chips. I could hear several people at the desk discussing Portillo’s, a well-known Italian beef joint in the area. That sounds good. Portillo’s and a beer.
Dr. DeBouw talked with Peg after he’d finished. My gallbladder was “ugly” and there were more stones marching down the cystic duct, so taking it out was prudent. He said surgery was “textbook” and took about 20 minutes. If recovery went well, I could go home later in the afternoon and have anything I wanted for dinner, even steak.
That sounded good, but someone hadn’t bothered to tell PACU or the floor to which I was going to be transferred. Normally, one goes from PACU to another outpatient area where the staff assesses one’s fitness to go home. “What we’ve got here is failure to communicate.”
Patient transportation took me to the fourth floor and dumped me off in a room the size of a storage closet. There was barely enough room on either side of the bed for one person. Someone had dutifully filled out the white board facing the bed with pertinent information like my nurse and her in-house phone number, my physician and what tasks had been scheduled for the next 24 hours. My new young nurse, Ashley, and her equally young assistant bounced into the room, bright-eyed and bushy-tailed, even though their shifts would end in a couple of hours. Ashley immediately hung a fresh I.V. bag (another one hundred fourteen bucks a bag and another $753/hour for the pump).
“Let’s get you settled in…” “Uh, I’m not planning on staying here for very long. Dr. DeBouw said I could go home this afternoon.” “Uh… Well, let me check on that. I thought you were going home tomorrow morning.” “Not if I can help it. I’ve been here long enough.”
She left the room, presumably to call my surgeon and confirm that I was indeed getting out of Dodge and returned in a few minutes.
“Yes, you can go home but before that you have to eat something, urinate and walk without difficulty.” “Ok, well I peed while you were gone. If you want me to walk, let’s go now!” “How about I have you order something from the menu, and we can walk while you’re waiting for it.” (Being able to order something charitably called “room service” is a recent development in hospital management. It’s still hospital food and sucks more often than not.)
Surgeons often inject long-acting anesthetic into the tissue around the trocar sites; I wouldn’t feel any pain until the following morning. I got out of the bed with little effort, grabbed the I.V. pole and led my nurse and her assistant out the door. I went down the hall and circled the nursing station at a brisk walk, the two of them marveling behind me as if Christ had just healed the cripple
“Well, just look at you go!”
You’re young and you think I’m ancient, but your perspective of age will change in about forty years. People in their sixties are no longer hanging out on Death’s doorstep. Neither are many people in their eighties.
My “dinner” arrived shortly after we returned to the room: desiccated grilled chicken and that tasteless broth I’d experienced the day before. The only saving grace was a small carton of Luigi’s Lemon Italian Ice. Very tasty.
Ashley bounced into the room again.
“We’re trying to contact the hospitalist because he has to approve your discharge?” “Why? The surgeon already discharged me. Why would the hospitalist care if I’m gone?” “Well, we just have to do it, but it shouldn’t be long. He’s already left the hospital but we’ll page him.”
After waiting another 45 minutes for the hospitalist’s blessing and satisfied that I met the criteria that would keep them from being sued for discharging me too early, they gave me the requisite discharge and follow-up information. Patient transportation wheeled me to the main entrance, stopping at the canopied walkway leading to the parking lot pickup point. He must have been tired after a long day.
“Can you make it from here or do you want me to wheel you out?” “Nope, I’ll take it from here.”
I got into the car and Peg drove off. We stopped by Walgreens and picked up my prescription for hydrocodone tablets (I used only one), then Portillo’s for a beef sandwich before going home to my own bed. But no beer.
Here’s the damage:
Description
Charges
Hospital
$47,914.92
ER Physician
$1,264.00
Medical Group Physicians
$1,850.01
Outside GI Consultant
$558.33
Surgeon
$2,900.00
Surgical Assistant
$1,450.00
Anesthesiologist
$2,475.00
CRNA
$2,475.00
Radiologist
$488.00
Pathologist
$73.00
TOTAL
$61,448.26
Medical charges May 4-6, 2021
I have good insurance which paid for most of this. We still had to pay more than $2400 out of pocket, but Peg is fortunate enough to have a Health Savings Account (HSA), which is funded with pre-tax dollars. I reached my deductible before the anesthesia group submitted its bill for both the anesthesiologist and the CRNA, $2475 each. So much for CNRAs being cheaper.
I can afford this but millions more can’t. It’s unconscionable that the richest country in the world won’t provide universal health insurance coverage. I don’t see that happening until Millennials and women run government.
Morning started at 6 a.m. with the Procession of Medications, a pill to prevent reflux, and my nurse noting my lipase level was down to 2,000. A tech took my temperature, blood pressure and pulse oximetry. The day shift nurse, Katrina, brought more meds around 7:30 a.m. which I took with the water I wasn’t supposed to be drinking.
“Uh, didn’t they tell you not to drink?” Nope, this is the first I’ve heard.
She also injected a dose of Lovenox®, an anticoagulant to prevent a deep vein thrombosis (DVT), because it had been ordered, not because I really needed it. I didn’t have the presence of mind to question it because I was tired but it seemed superfluous. My risk for a clot was low since I hadn’t had major surgery, I wasn’t bedridden, I don’t smoke and I’m not pregnant. Yeah, I’m old and fat but so what? (I refused it the next day, which is good because that little sucker was $119!)
An hour later a woman from Respiratory Therapy, who looked and talked like the commandant at a German women’s prison, appeared with one of the newer brand name steroid/long acting bronchodilator inhalers. Remember what I said about hospital meds costing a lot more? This one retails for about $450 and lasts 14 days; the hospital charged $570. My generic version, which lasts a month, is $40 with GoodRx®.
“I have an inhaler for you and I’m going to teach you how to use it. You pull back the cover and it’s very important that you hold it correctly with the vent side up. Then you take a deep breath and hold it.”
I pulled out my albuterol rescue inhaler. “I’m a physician. I’ve been using inhalers for a long time.”
She snapped at me. “You should NOT have your own inhaler! We are responsible for you and must know every medication you are taking! Another respiratory therapist would turn you in.”
Now she reminded me more of General Burkhalter from Hogan’s Heroes. Turn me in? What is this, Stalag 17? Are you going to send me to the Russian Front?
She watched while I inhaled like toking from a bong, then put it in a plastic bag which she placed on the shelf below the TV. “Someone will come back tomorrow for your next dose.” You think I’m so stupid that someone has to watch me?
No, it’s because the hospital can charge $424 to “administer” the medication and $323 to “demonstrate” how to use it! What the hell do people without insurance do with those kinds of charges?
The Parade of the Grey Coats began around 9 am. Doctors (usually men) in white coats often cause spikes in patients’ blood pressures, so now most wear either grey or blue lab coats to minimize the psychological trauma. Or maybe it’s because white coats are a bitch to keep clean. (I have a royal blue lab coat with a Grateful Dead patch on the pocket.)
The internal medicine hospitalist showed up first. Now, I’m not sure what a hospitalist does other than generating revenue and confusion while making it possible for office-based internists to never set foot in the hospital. I’m sure I’ll get a lot of shit for that but my sister-in-law’s experience with hospitalists, who are usually much younger than the seasoned staff physicians, was exasperating.
He asked me to recount the events that ended with my admission, the third request if you’re keeping count.
“How are you feeling?” “Better than when I came in.” “Well, your lipase levels have come down nicely to around 2,000 with the I.V. fluid flushing it out. Do you mind if I examine you?”
He poked my abdomen in a few places. “Does that hurt?” “Not much but you’re not as rough as the ER doc last night. Do you know Dr. Nell?”
He chuckled, “Yes, I like her, but she can be a little, uh, enthusiastic.” That’s a polite way of putting it.
“Your lipase levels suggest you have pancreatitis. You’re not an alcoholic and you don’t smoke so it’s likely caused by gallstones. That pain you had may have been a stone passing, especially since it didn’t last too long and you’re feeling better. I’m going to order an ultrasound of your gallbladder. We might be able to send you home later today, but we’ll have to wait for the GI guy to see you.”
We interrupt this tale for a moment of education and enlightenment.
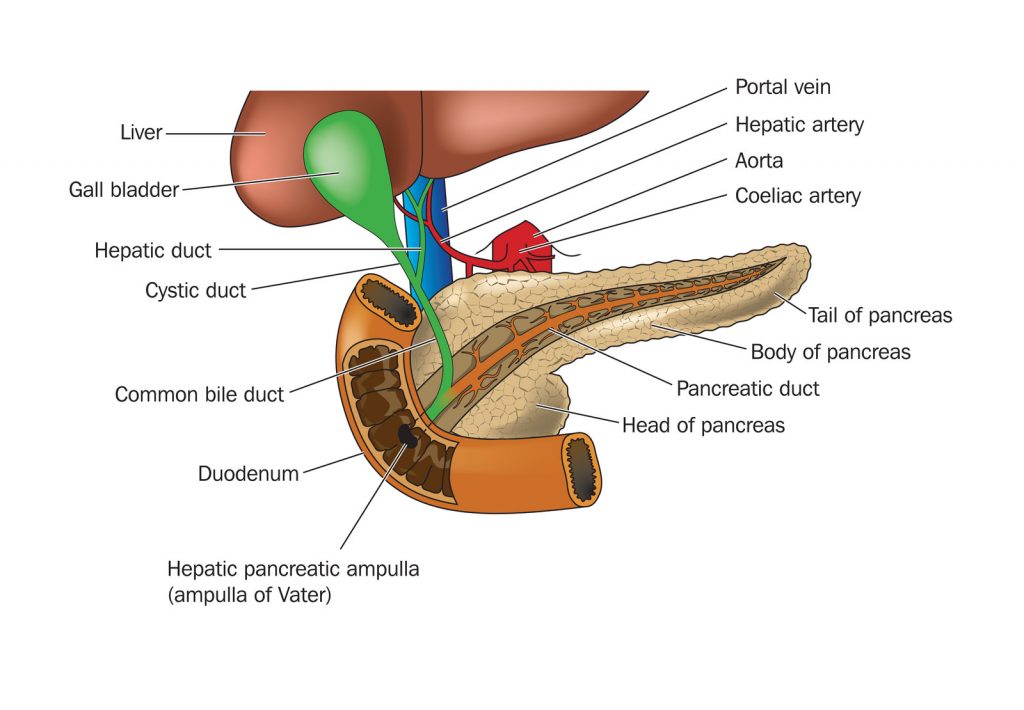
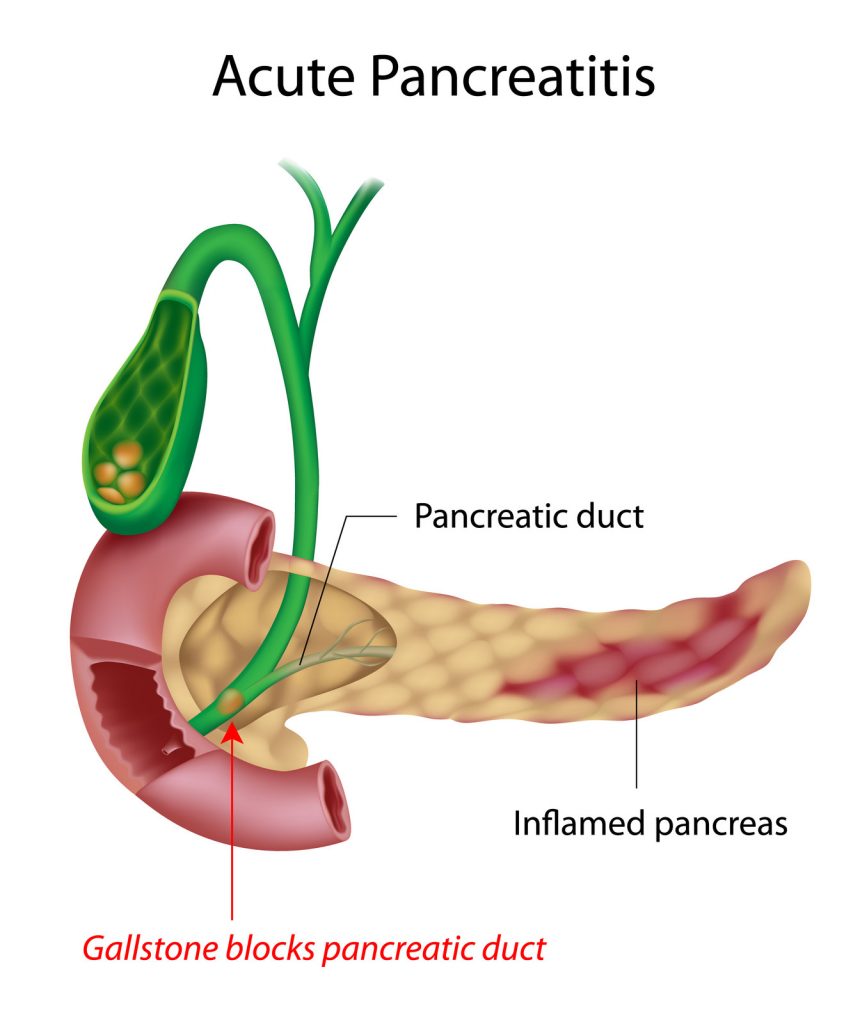
THE PATHOPHYSIOLOGY OF BILIARY PANCREATITIS
The gall bladder is a pear-shaped organ that lies below the liver. It stores and stores bile, which digests fats. Bile leaves the gall bladder through cystic duct. The pancreas also secretes digestive enzymes through the pancreatic duct which joins the cystic duct, forming the common duct. Both empty into the duodenum through the hepatopancreatic ampulla, also known as the Ampulla of Vater (Darth Vater?), which is controlled by the Sphincter of Oddi. Sounds like something out of Norse mythology.
The gall bladder also provides a source of income for general surgeons when it becomes inflamed (cholecystitis), full of stones (cholelithiasis), or both. Stones form when, for unknown reasons, stuff in bile crystalizes and forms gallstones, in much the same way stuff in urine crystalizes to form kidney stones. If a stone gets stuck in the common duct, it blocks secretions from both the gallbladder and pancreas, resulting in gallstone pancreatitis, which is what I had. Pancreatitis can also result from excess alcohol consumption, smoking, prior abdominal surgery, obesity, infections, injuries, and pancreatic cancer.
Abdominal ultrasound is the easiest way of finding gallstones and often cholecystitis, as inflammation thickens the gallbladder wall. Other, and far more expensive, diagnostic methods include nuclear medicine scans, Magnetic Resonance Imaging (MRI), or Endoscopic Retrograde Cholangiopancreatography (ERCP), looking directly into the duct with an endoscope.
A common home test for cholecystitis is consuming a greasy meal which results in excruciating upper abdominal pain; however, this is not medically recommended.
Now, back to the program already in progress
Peg arrived around 9:30am.
Did I ever mention Peg hates hospitals? No, she REALLY hates hospitals. Her mother said, “Hospitals are where you go to die.” If Peg has the big one at home, she wants me to just hold her hand and stroke her arm until she passes. Then, and only then, can I go through her office looking for the lam money.
She also thinks there is a lot of waste and abuse, albeit mostly inadvertently because no one thinks about cost in a hospital. This is largely true. I worked for a staff-model HMO thirty-five years ago. “Managed care” was withholding care from patients for profit and employed physicians weren’t good enough to work with “real doctors.” Forty years later most physicians are employed by heartless entities, and I got the last laugh.
“So, what’s happened so far? I talked to your nurse about 5:30 this morning and she said you had a good night.”
“Yeah, my lipase level has come down to two thousand something. I saw the hospitalist earlier; he thinks I have pancreatitis from passing a gallstone. He ordered an ultrasound and said I might get to go home…depending.”
“Do you have any pain?” “No, I feel pretty good right now.”
Just then a guy from Patient Transportation appeared in the doorway. He took me down for ultrasound on my bed, reversing the previous night’s course. I stared at the ceiling again as we went left out of my room, into the elevator, down to the first floor, out and a couple of left turns before backing me into a cramped ultrasound exam room. The ultrasound tech introduced herself, squirted warm ultrasound gel on my abdomen and started the exam. About fifteen minutes later she finished.
“And….?” “You’ve got gall stones, but you didn’t hear that from me.” “My lips are sealed.”
As the transportation guy wheeled me out someone from nuclear medicine said: “We’re going to see you later.”
Once back in the room I told Peg what we’d both suspected. Then the gastroenterologist showed up – not exactly a fount of wisdom. At his request I repeated the events of the previous 12 hours for the third (or was it the fourth) time. He pushed on my abdomen, and I winced.
“Well, at least it’s in the right place. Your ultrasound showed you’ve got gallstones. We’re going to get a CT (Computed Tomography) scan to confirm the diagnosis and a general surgeon will see you later today.”
“Ok, how about not giving me another liter of fluid? I’ve had three in the past ten hours, and I’ve been peeing every two hours.” “Yeah, that’s probably a good idea. We’ll also try you on clear liquids.”
Peg and had a discussion after he left.
“You told me it didn’t hurt, and you told him it did.” “It didn’t hurt when you asked me. It hurt after he reefed on it because it’s inflamed, not because I’m lying to you.” “Getting a CT scan to confirm what we already know is a waste of money! The ultrasound showed you have gallstones; a CT scan is redundant. It’s not going to give any better information. And THIS is why healthcare is so expensive!”
Peg had a point. If you’ve already made the diagnosis with a $1,000 ultrasound scan, why tack on another $3,000 for a CT scan to tell you the same thing? If an ultrasound might be difficult because of extreme obesity, then just do a CT. (Side note: Later that day the general surgeon told me the CT scan was used because ultrasound can’t evaluate the pancreas very well for things like fluid collections or tumors, which is important when considering surgery.)
We saw the cardiologist next and recited my history for the fifth time. I recognized his name; he is the “electrician” who did my sister-in-law’s cardiac ablation. She absolutely loves him, and his partner is my cardiologist, so I trusted whatever he had to say.
“Your EKG and troponin levels were normal. You haven’t had a recent stress test and we’ll have to clear you if you’re going to have surgery.”
I had a stress test in 2017 because I’ve no reliable family history and I was going to start work as a hospitalist. Unfortunately, a normal stress test doesn’t mean you won’t drop dead a few weeks later like Tim Russert.
There are two ways to do a stress test. The time-honored tradition is to hook a patient up to a 12-lead EKG, run him or her on a treadmill until the pulse is at least 130, and see what happens. ST segment changes suggest coronary artery blockage. (So does grabbing one’s chest and having the big one.) The test runs a few hundred bucks.
The other way is a cardiolite stress test, injecting the subject with a radioactive tracer and scanning the heart before and after the treadmill. A decrease in uptake after exercise suggests blockage and may indicate which artery/arteries are affected. The tracer and scan add several thousand bucks to the procedure, even though it is of questionable benefit in someone who has no history of coronary artery disease. Coronary angiography, injecting dye through the coronary arteries, is still the definitive test for detecting blockages.
The charge for an outpatient study is considerably less than doing the same thing in a hospital:
Item
outpatient
inpatient
Treadmill
$325.00
$1,200.00
Tracer
$720.00
$918.00
Scan
$1,634.00
$5,532.00
Interpretation
$300.00
$300.00
TOTAL
$2,979.00
$7,950.00
Cardiolite Stress Test: Comparing outpatient and inpatient charges
A nuclear med technician came in with a syringe containing the isotope in a shielded container and transportation took me down in a wheelchair instead of a gurney. This time I could at least see where I was going. The cardiac evaluation unit was below the first floor and reminiscent of the Batcave.
One of the women in the scanning room explained the procedure, then had me lay on the slightly uncomfortable scanner bed. The initial images took about six minutes, then they wheeled me across the hall to the treadmill room. Another tech applied twelve more EKG leads on my chest and abdomen, on top of the six leads I had for the portable monitor. The woman running the test explained what was about to happen.
“You’ll be on an incline on the treadmill. It will start out slowly for a few minutes, and then I’ll increase the speed until your heart rate gets to 130. You’ll have to keep that pace for at least a minute. Try to go as long as you can. When you need to stop, I’ll slow the treadmill for a one-minute cool down phase. I see you have exercise-induced asthma. Do you have an inhaler?” “Yes, I do but the respiratory Nazi told me I shouldn’t have it in the hospital.” “Well, she’s wrong; we like treadmill patients to have their inhalers on hand.”
Left hand, have you met right hand?
The incline was fairly steep, more than I’ve ever tried at home. I held onto the bar across the front of the treadmill to keep from falling backwards. The pace was manageable despite feeling I was hiking up a mountain.
Then, to quote Emeril Lagasse, she “kicked it up a notch.” Actually, several notches. It didn’t take long for me to hit the target heart rate. I managed two minutes at that speed before I told her I had to stop.
“Are you having any pain or trouble breathing?” “No, I’m just way out of shape and too old for this shit.”
I went back into the scanner for about three minutes before being wheeled back upstairs. I napped for a while, while Peg sat in the corner playing with her Kindle and looking at the news feed on her phone. I figured no news was good news.
The day nurse came in a little after 1pm to tell me the CT scan was scheduled for around 4pm and I’ll get oral contrast to drink around 3pm. The guy from transportation arrived a little before 4, followed by the nurse.
“Wasn’t I supposed to drink some contrast?” “Uh, you didn’t get it?” Would I be asking you if I had?
She sputtered a bit and disappeared, possibly to give someone an ass-chewing, and to get the CT scan rescheduled. Peg rolled her eyes.
“If you were just a regular patient, you would have gone for your scan without asking any questions. They would have done the CT, discovered you didn’t have the oral contrast, and sent you back upstairs, and repeated it later. And you wonder why I hate hospitals.”
I saw the surgeon around 6:30, after Peg had gone home to feed Baxter. We hit it off immediately. He extolled the virtues of removing gallbladders with a laparoscope and I told him about assisting on an open cholecystectomy when I was an intern. Back then they made an autopsy incision from the breastbone along the right rib margin, then pried the muscles apart to get to the gallbladder. The guy I helped with was fat and needed a very large retractor called a Joe’s Hoe for exposure. Yeah, it looked like one could till soil with it.
“There are two options. The first is to have the surgery since you are already in the hospital, and you’ve gotten cardiac clearance. The other option is letting you go home and scheduling this as an outpatient. I’d recommend doing it now because we know you have gallstones and you’re likely to have another attack within three months. It’s better to take care of it now, because I’ve seen people wait and then come in with a necrotic gallbladder. They end up in ICU on I.V. antibiotics and sometimes a ventilator because they are really sick.” “My wife works long hours. I need to talk to her and make arrangements. What is the chance of passing another stone in the next two weeks?” “It’s likely pretty low but not zero. You might want to just get it over with.”
Well, that sounded good to me; I wouldn’t have a lot of time to think about going under again. We talked about my prostatectomy; he said taking out my gallbladder wouldn’t take as long, and I could probably go home a few hours later.
“I know your surgeon. We’re actually very good friends, even if he did go to Ohio State.” Oh God, he’s a Wolverine. They can be sooo insufferable! But he seems like a decent guy.
“In the meantime, you can have a clear liquid diet tonight. Don’t have anything after midnight in case you decide on surgery. I have one case in the afternoon.”
I called Peg.
“He said we can do it now or do it later. I told him you had to work and could we do it in a couple of weeks. He said we could but there was a chance of another attack before surgery.” “Well, what do you want to do?” “He’s coming back in the morning and you’ll probably be here before him, so you can ask him any questions. If I do it tomorrow, I won’t have a lot of time to think about it.” “I’ll go along with whatever you want.”
Katarina brought me two cups of contrast just before 7pm.
“Drink these now and I promise you’ll be downstairs for your CT scan around 8pm.” Well, this better happen!
Someone arrived just before 8pm and took me down to the CT room. It was cold, probably to protect the equipment which can become very warm. The tech who met me was a scruffy guy who reminded me of the dude that drove the school bus down to the water when a bunch of us went canoeing at Turkey Run State Park in Indiana during college. (His “mandatory safety instructions” were “If the brakes go out on this bus, put your head between your legs and kiss your ass goodbye!”)
“Marian will help you lay on this skinny bed while I get everything set up. I’ll let you know when I push the I.V. contrast because your head will start to feel warm and then you’ll think you’ve peed your pants. You’ll have to hold your breath a few times but that doesn’t last long. Do you have any questions?” “Nope, let’s just get this done.”
The scan was as he described. I held my breath a few times while the scanner did its thing. The I.V. contrast created a brief sensation of warmth in my head and nether regions, passing quickly. I was back upstairs by 8:30 and I called home to say goodnight to Peg and to Baxter, who wasn’t taking this very well at all. He paced Tuesday night until 2am and this promised to be another fitful night.
Maybe tomorrow would bring a reprieve from all this fun and excitement.