(Note: I’m taking a short break from the Iceland travelogue.)
Peg and I went to Galena, IL, a quaint town cum tourist trap in the northeastern corner of Illinois, just across the Mississippi River from Iowa. One of our food destinations was a supper club in East Dubuque.
Anyone who lived in the Midwest in the middle of the 20th century is familiar with the supper club. Initially an alcohol workaround during Prohibition (private clubs could sell liquor to members), supper clubs became social destinations during the 1940s through the 1960s. They were family-owned restaurants often on the fringes of rural towns and provided patrons with the classic evening out. One started with cocktails at the bar followed by dinner and ended with after-dinner drinks and dancing.
Men often ordered an Old Fashioned: simple syrup or a sugar cube dissolved in a bit of water, bitters, ice and bourbon or rye, garnished with a Maraschino cherry. Others popular drinks were the Manhattan (rye or bourbon, sweet vermouth, bitters and the cherry) or the classic Martini (gin and dry vermouth garnished with a pimento-stuffed green olive or lemon twist). Cream drinks were popular after dinner, mostly among women, and were often made at home with ice cream when blenders became affordable.
Classic Cream Drinks •Brandy Alexander: brandy or cognac, crème de cacao, cream. •Pink Lady: gin, applejack, lemon juice, grenadine and a small egg white, shaken and garnished with a Maraschino cherry. •Pink Squirrel: crème de Noyaux (or Amaretto, but it won’t be pink), crème de cacao, cream. •Grasshopper: crème de menthe, white crème de cacao, cream.
The dining experience was very predictable. While perusing the menu, the waitstaff would bring a relish tray with carrot and celery sticks, diminutive sweet pickles, olives, radishes and green onions along with packets of Club Crackers and those dry “breadsticks,” served with a dipping sauce or a spreadable cheddar we knew as “Bar Scheeze.” One could get shrimp cocktail or oysters for an appetizer.
Entrees were traditional American cuisine: steaks, chops, and chicken. Supper clubs usually had the Friday Night Fish Fry and Prime Rib on Friday and Saturday nights. Meals came with soup and salad (iceberg lettuce, a strip of carrot, a little red cabbage, maybe a tomato slice). Salad dressing options were usually oil and vinegar, Thousand Island and French, which you spooned from stainless steel three-bowl condiment server the waitstaff whisked from one table to another. The classic baked potato with sour cream and chives was standard. All this came with hot bread or rolls and butter.
Dessert and coffee came after dinner and before dancing. Any leftovers went into a paper “doggie bag,” often imprinted with a happy cartoon dog. There were no polystyrene containers or foil trays with non-recyclable plastic lids.
My brother-in-law’s mentioned Timmerman’s Supper Club in East Dubuque, IL when he heard of our plans. He and his sons often go to the casinos in Dubuque during their annual golf outings at Eagle Ridge in Galena. “It sits on a bluff overlooking the river. Zimmerman’s or something like that. We’ve never been there but maybe you can check it out.” (I didn’t know that Peg had already made a reservation.)
We headed west towards East Dubuque on US-20, a four-lane running through rolling hills. We’ve had a warm summer and early fall, so there was very little color in the trees; it would probably be spectacular in another two weeks. About twenty-five minutes later we turned on to Timmerman drive, a rather steep hill leading to a cemetery on the left and a ridiculously large parking lot on the right. I let Peg out under the canopy at the entrance before parking and joining her.
It was like going back in time 60 years! Think of Kellerman’s from Dirty Dancing.
The building is brick and concrete block, painted a warm cream color. There are portraits of the founders in the entry, above the wheelchair lift. Wrought iron railing, covered with many years of paint, lead up the stairs and along the waiting area. The doors and trim are all a dark walnut; the swinging doors to the kitchen have the old diamond windows.
The dining room is the size of a basketball court with high ceilings, laminated wood beams and acoustic tiles on the ceiling. There’s a large, blue sailfish mounted on the wall above two large china cabinets. Enormous plate-glass windows in aluminum frames, tilted out about five degrees from the vertical and running from the ceiling almost to the floor, look out over the Mississippi. Bluish sunscreens and motorized canopies shield patrons from direct sunlight until the sun goes down, when the staff retract them to maximize the view.
There are large valances running the length of the windows, with narrow tied back largely decorative drapes hanging about every 10 feet. I noticed three of the old wood and black grille loudspeakers mounted near the ceiling.
Tables seating two to eight people are positioned strategically throughout the dining room, allowing the waitstaff to move among the maximum 200 guests with grace and style. There is a half-wall in front of the kitchen entrance, topped with a decorative wooden lattice. The Palisades Room, to the left of the main dining room, has a private bar and is available for social events. (I suspect it was used for dancing during Timmerman’s heyday.)
The wait staff are all dressed in black. The high-school aged busboys wore black pants, long-sleeved white shirts and black bowties. They reminded me of my days bussing tables at the Lamp Lite Room at the Bowl-Mor in Streator, IL, minus the bowtie.
The hostess took us to our table and left us with menus, large, faux-leather-bound things with printed pages inserted into stitched plastic protectors. After we were seated our waiter gave each of us a slice of cornbread and took drink orders. Peg wanted a dry Beefeater martini with extra olives while I went off the board and got the Pomegranate Martini (citrus vodka, triple-sec and pomegranate juice) instead of the usual gin and tonic. We ordered the stuffed mushroom appetizer while perusing the menus; the aforementioned complimentary relish tray now cost nine bucks. Nostalgia ain’t cheap!
We toasted twenty-five years of marriage, having done that without strangling each other and defying the odds a couple of people had given us, as we watched the sun set over the river.
Peg ordered a ribeye with a baked potato (with sour cream, of course); I opted for the fried walleye and wild rice medley as the only time to get walleye at home is at Culver’s during Lent. Peg’s steak came on the classic sizzling steak tray, the wooden base darkened by the heat of many years. My walleye took up the entire platter; the rice came in an oval side dish.
Our waiter cleared the table once we’d finished, and Peg’s leftover ribeye had been saved in a black takeout container. He then brought us an anniversary dessert-a warm chocolate chip cookie drizzled with chocolate and caramel, topped with a scoop of vanilla ice cream and a single birthday candle.
Getting back to Galena was a bit challenging. We had to make a right turn (the median made turning left impossible), which took us over the bridge into Dubuque. I turned onto US-61, missing the first and only opportunity to loop back around to the bridge. We passed by Q Casino before crossing over another bridge into Wisconsin and then back into Illinois on a winding two-lane. We were finally pointed in the right direction and made it back without hitting a deer on the now pitch-black highway.
It was a perfect conclusion to a memorable weekend.
As we pulled into each port, we were awakened every morning by the cheery voice of our Cruise Director, Katy Syrett, a dark-haired Scottish beauty who also sings and dances in the after hours. It reminded me a bit of the daily announcements that greeted Patrick McGoohan in The Prisoner, without the sinister undertone.
Ísafjörður (“ee-sa-fyo-tthur”) is the largest town in the Westfjords, which is relative, given only 2,700 people live there permanently. It is located on the Skutulsfjörður (“skoo-tuls-fyo-tthur”) fjord, a branch of the larger Ísafjarðardjúp (“ee-sa-fyo-tthar-djup”) fjord. In 2023 Ísafjörður extended the port to accommodate larger cruise ships, but also set a limit of 5,000 passengers disembarking per day to avoid overwhelming the town’s resources.
Our ship docked near the Naustahvilft Troll Seat, (“noy-stah-klift”) a large depression in the mountains next to the fjord. According to legend, sunlight turns trolls into stone and Naustahvlift was created when a troll hid in the hollow in the cliff to avoid the approaching dawn. Her enormous weight turned it into a seat; the adventurous can hike the trail and take in a spectacular view of Ísafjörður.
Today’s activity was touring Ísafjörður and Bolungarvik (“bol-un-gar-vik”), a small fishing village about 8 miles north. We disembarked from Deck A, the lowest passenger-accessible deck, this time through a narrow corridor and on to a long ramp with a very slight decline. Getting back on the ship was a bit of a nightmare as we ran into people headed out for the next tour. After that, the staff started staggering departures and arrivals.
Our tour guide was a pleasant and amusing young man from the U.K. who was far easier to understand and more personable than our native Icelandic guide on Sunday. We passed by two men loading a stretcher into a hearse as we were leaving the dock. I don’t think it was anyone from our ship, but you never know.
The bus meandered through the narrow village streets, past small guest houses and hotels in the city center. Our guide pointed to a construction site where Ísafjörður is adding land mass into the harbor to build student housing for the University Centre of the Westfjords, whose enrollment increased substantially after COVID restrictions were lifted.
We headed out of town on the narrow highway hugging the shoreline. We saw four large, circular structures jutting out of the water; these are open-net salmon farms which contribute to the economy, but at a cost. Farmed salmon have escaped from the pens, threatening the survival of wild salmon, whose global numbers have been dwindling. Sea lice and the pesticides used to treat them, along with the salmon’s own waste, pollute the water and may cause dangerous algae growth.
The bus entered the Bolungarvíkurgöng (“bol-un-gar-vik-uhr-gung”) Tunnel a few miles further along the road. The tunnel, 5.4km/3.36mi long, was opened in 2010, bypassing the treacherous coastal road which was susceptible to rock falls and avalanches from the Óshlíð (“ohs-lith”) mountains. The tunnel is well lit and there are turnouts along the way for passing.
Entrance to Bolungarvíkurgöng. Christian Bickel, 2011.License CC BY-SA 2014
The Vestfjarðagöng (“vest-fyar-tha-gung”)Tunnel, west of Ísafjörður, is the longest tunnel in Iceland and has three arms which meet in the middle. That would have been an intriguing sight!
Entrance to Vestfjardargöng. Bromr, 2009. License CC BY-SA 2014
Trolls, elves, monsters and ghosts are part of Iceland’s storytelling heritage. Most Icelanders hedge their bets and won’t openly deny their existence…just in case. So, when the Bolungarvíkurgöng tunnel was being excavated, the construction workers started the day by apologizing to the trolls within the mountain for disturbing them…just in case.
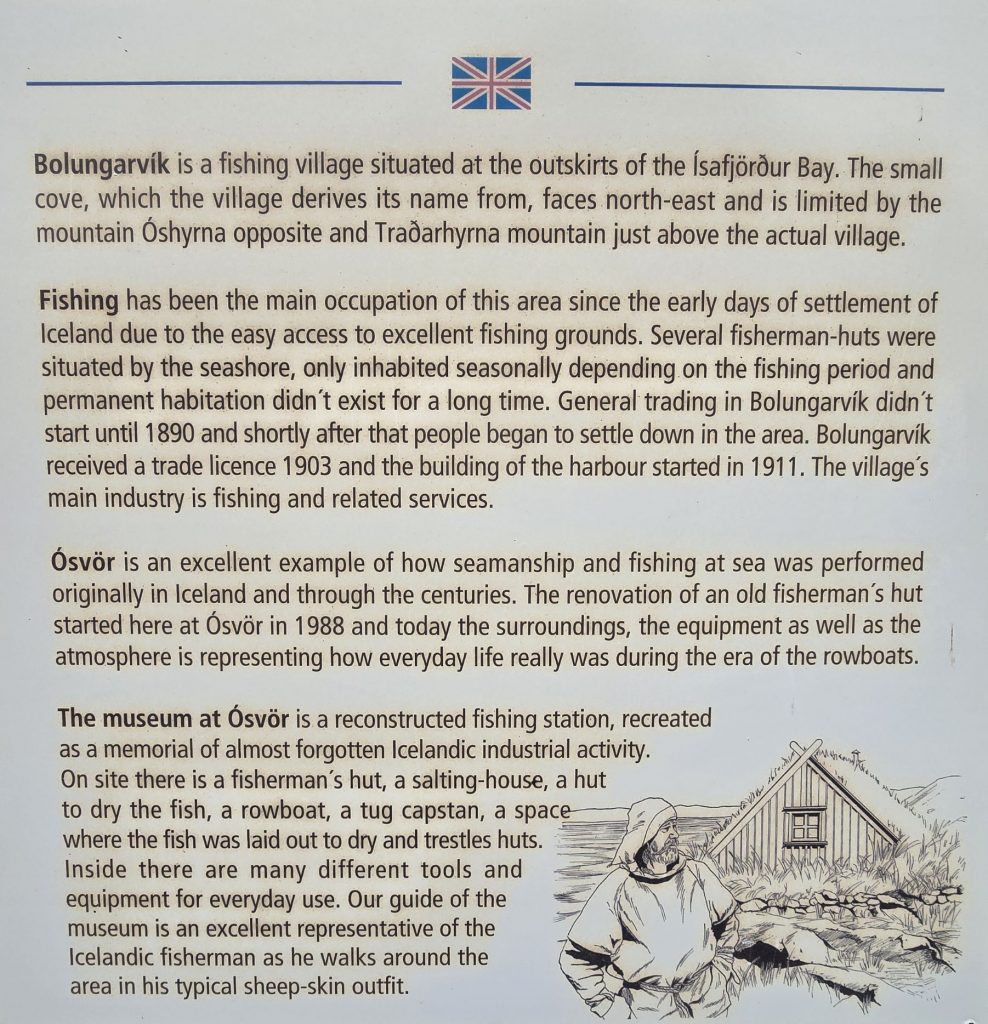
Bolungarvík is a small coastal village (pop. 1,022), founded in 940 AD. It was one of the largest fishing stations in Iceland for centuries. Fishing and fish processing became the primary source of income at the end of the 19th century. The town was inaccessible except by boat until 1950 when the first road to the village was completed. Between April and September sport fishermen flock to Bolungarvík angling for cod, redfish, haddock and halibut. (The average halibut is 100kg/220lbs!)
Bolungarvík
Plaque at Ósvör Maritime Museum
According to legend, Þuríður (“thur-ee-thur”) Sundafyllir and her brother, Þjóðólfur (“thyo-thol-fur”), the founders of Bolungarvík, got into a pissing contest after Þuríður granted her brother all the land he could fence in one day. Þjóðólfur didn’t fence as much land as he’d anticipated and became angry when his sister wouldn’t let him have any more. Out for revenge, he tried to steal one of Þuríður’s oxen, but she caught him.
The siblings were also sorcerers and cast spells on each other. Þuríður said, (and I’m paraphrasing), “Yo, sheep dung for brains! For trying to steal my ox, you shall become a rock that birds will defecate on for eternity!” Þjóðólfur turned to stone and fell into the bay, where birds shit on him until 1936 when, according to the locals, he mysteriously disappeared.
Þjóðólfur retaliated. “You wanna play that game, bee-yach? YOU shall forever become a rock where the winds blow the strongest.” And with that, Þuríður turned into a stone that sits at the top of Óshlíð. How he managed to cast a spell when he was already turned to stone was never explained in the legend.
We drove through town and stopped at Félagsheimilið Bolungarvík, (“fya-lath-shay-mi-lith”) the town’s community center, where a local musician performed two of his own compositions. The first was about an obscure wrestling tradition, (possibly Glíma (“glee-ma”), but I wouldn’t swear to it) and the second lamented the long Icelandic winters. Both were in Icelandic, so we couldn’t understand any of the lyrics, but he was passionate.
We reboarded the bus and on our way out of town our guide talked about the Arctic Tern, a bird that one site described as “so graceful and yet such a nuisance.” Instead of picking secluded areas, terns build their nests wherever the hell they want and become very aggressive if an unsuspecting human wanders near the eggs. They will dive bomb one’s head and, if they are particularly miffed, shit on you for good measure. Our guide was once attacked trying to draw the terns away from the tourists in his charge.
The bus turned around across from Óshólar (“oh-sho-lar”) Lighthouse and drove back to the Ósvör (“ohs-vur”) Maritime Museum, a 19th century replica of a fishing station. There are three small buildings: a fish drying platform, a salting shed, and crew quarters with tools. An old fishing boat sits on the beach. The museum’s guide is dressed in traditional sheepskin fishing gear, minus the fish oil waterproofing actual fishermen used, which gave it an offensive smell! The path to the buildings was rocky and somewhat steep, so we skipped this part of the tour. (Note to self: next time bring the walking sticks you packed!)
Traditional Fisherman, Bolungavík, Iceland. TommyBee. Public domain
The bus took us back into Bolungarvík where we turned around again and headed back to Ísafjörður. We went through the town center, past the local hospital and Íþróttahúsið á Torfnesi (“ee-throw-tha-hoo-sith”), the Torfnes Sports Hall, then west out of town to the Bunárfoss (“boo-nyar-foss”) Waterfall in the Tungudalur (“toon-goo-tha-lur”) Valley, where our guide promised us we would sample a glass of the purest water in Iceland.
Bunárfoss is not as spectacular as Seljalandsfoss or Skogafoss, but it’s still impressive. The more physically fit can climb 80m/262ft to the top of the falls for a view of the valley below. The waters continue in a gentle brook.
Bunárfoss Waterfall
Downstream from Bunárfoss
We got off the bus and the driver handed us plastic cups while our guide filled a restaurant style plastic pitcher with water from the stream, doling out samples to the curious. He then noted the water was so pure because there were no sheep in the mountains to contaminate it. It tasted remarkably like…water.
Our group, waiting to sample the waters.
Foliage at Bunárfoss
Thirst quenched, we handed our cups to the driver and boarded the bus. Satisfied we were all accounted for, our guide told us a tale about a different tour.
“Before leaving, the driver asked if anyone was missing. No one spoke up so he pulled out of the parking lot. Just then he noticed a woman in the road behind him, waiving her hands frantically. He stopped and said ‘I thought no one was missing.’ A man a few seats back said, ‘That’s my wife. She’s always late for everything, so I thought this would teach her a lesson.’ “
Dead man walking…
On our way back to the ship we passed the Tungudalsvöllur (“toon-goo-tha-lur-vote-lur”) Golf Course: 9 holes, par 70 and a three-month season. Probably the only thing my brother-in-law would find worthwhile about this trip.
Tungudalsvöllur Golf Course
I investigated “Things to do in Ísafjörður” when I began this blog post and discovered there are two ski resorts on the mountains above Bunárfoss. Tunguladur, for downhill skiing, has 3 lifts and a ski lodge. Seljalandsdalur (“sel-ya-lands-da-lur”) is for cross-country skiing. I’m writing this during the second week of September and Ísafjörður already has snow and winter weather warnings!
Easter in Iceland is a five-day national holiday, from Holy Thursday until Easter Monday, and an opportunity for the hardy to “…flee to Iceland’s winter resorts where they ski from dawn until dark, get wasted on Black Death eat buried shark and boogey until breakfast.” (Black Death is Brennivin, Iceland’s version of aquavit, a variety of herb-flavored liqueurs that are not for the faint of heart. Chicago’s ghastly Jeppson’s Malört is another version of aquavit.)
We had signed up for the “Panoramic Southern Coast of Iceland” bus tour, partly because the activity level was described as “easy,” but that was a big mistake. It turned into nine exhausting hours of getting on and off a bus, hiking across rocky paths (which limited Peg’s exploring), and enduring an obnoxious, older (60s) but completely able-bodied couple who defiantly were the last to get back on at each stop, despite our guide’s repeated warning, “We are on a tight schedule.”
The tour bus left at 7:30am; it’s a good thing we had gone to bed early and had adjusted to the time difference. Room service arrived at 6:30am; I grabbed one of the bathrobes to avoid opening the door stark naked. We had a delicious light breakfast, then grabbed our jackets, the QuietVox modules, and Peg’s Rollator, and headed for the elevator. We scanned our room cards at the ship’s exit point, walked down the ramp and through the terminal checkpoint, and then stood in line outside waiting for our bus. Getting off the ship was much easier this time as we were at low tide, and the ramp wasn’t as steep.
Our bus was the third in line, and we were afraid we’d have to walk to it, but the first two buses departed and ours took their places. The bus driver loaded Peg’s rollator under the bus and our tour guide took our tour passes and welcomed us on board. We headed for a pair of seats in the middle of the bus. Before we left our tour guide had us turn our QuietVox sets to Channel 3 and made sure we could hear her through the headphones. (One of the tourists later deduced the channel always corresponded to the bus number.)
One might be forgiven for expecting the bus to have nice, comfy wide seats with generous leg room as seen in movies. Our seats were closely spaced, firm and built for skinny Europeans instead of fat American asses-worse than airline steerage class. The seatbelts were barely long enough and trapped us in uncomfortable positions. After the first rest stop, we moved to the five seats along the back and had much more room.
It was overcast and drizzly as we headed south from the terminal to Route 49, then east to Route 1, known as the Ring Road because it circles the entire island. After several minutes the outskirts of Reykjavik disappeared, and we were in the rugged countryside. Our guide pointed out steam coming from thermal vents near the road.
A thermal vent by Route 1
Geothermal energy provides Iceland with about twenty seven percent of its electrical power; hydroelectric power makes up the rest. Superheated, acidic steam collected from deep wells powers electrical turbines. Heat exchanges warm the water that is used to heat about 86% of Iceland’s homes and businesses. And geothermal water provides Iceland with its famous spas. (The Blue Lagoon isn’t a natural formation; it was created when the Svartsengi Power Station released geothermal brine was released into the lava field.) The guide at our last stop, the Lava Centre, told the group that his monthly electric bill is about eight bucks because electricity is so cheap.
We passed an airfield marker which seemed completely out of place as there were no visible hangers or aircraft. I discovered this is the Sandskeið glider port; here’s a video of a glider in flight. (Seriously, someone tell me when Iceland has sunny days, because it never looked like this during our trip!)
Hveragerði The mist turned into fog as we gained a few hundred feet in altitude, then dissipated as the highway descended towards Hveragerði (pronounced: KVER-ah-ger-thhi). An earthquake in 2008 devastated much of Hveragerði; when the town rebuilt, it expanded its greenhouse industry, becoming Iceland’s “greenhouse capital,” providing the island with fresh produce year round, including tomatoes, cucumbers, strawberries, lettuce, red and green peppers, mushrooms, herbs and cut flowers. Carrots and potatoes grow outside in geothermically warmed soil. One can tour the Friðheimar family farm, learn about greenhouse production, enjoy fresh tomato soup, fresh tomatoes with Burrata cheese, and visit Icelandic horses in the farm’s stables. (Do not, under any circumstances, refer to them as “ponies!)
Selfoss We crossed the Ölfusá river into Selfoss, a commuter town about 30 miles from Reykjavik. Selfoss means “Seal Falls” in English, but there are no seals and no waterfalls. It’s a pity we didn’t stop here because the town has a lot to offer. Having also suffered significant damage from the 2008 earthquake, Selfoss rebuilt a New Downtown, a vibrant, pedestrian-friendly area with shops, restaurants, and recreations of buildings from Iceland’s past, like the Old Dairy Food Hall. Skyr, the thousand-year-old Icelandic yogurt, is mostly made in Selfoss. The Bobby Fischer Center houses memorabilia of 1972 chess champion, who lived in Selfoss from 2004 until his death in 2008.
Aerial View of Selfoss
Hvolsvöllur From Selfoss we headed east, stopping in Hvolsvöllur (pronounced “Kvols-vol-yur”) for a bathroom break at the N1 fuel and charging station’s Nesti grill. The bathrooms are exceptionally clean, and the staff is very friendly. I bought a couple of water bottles and some chocolate. We would stop at the Lava Centre here on our way back, but it would have made more sense to do it first, since we were exhausted by that time. We continued on to Seljalandsfoss Waterfall.
Sheep May Safely Graze We saw sheep grazing along the highway, sometimes on the wrong side of the fence. There are an estimated 500,000 to 800,000 sheep in Iceland, outnumbering the human population. Icelandic sheep were susceptible to diseases introduced by selective breeding in the 19th century so now importing sheep is illegal. The subsequent isolation produced a very pure strain, and Icelandic wool is unique-and scratchy! Peg’s hand became very irritated after feeling a sweater in one of the gift shops.
Sheep breeding begins in November; they give birth in May, a time known as Sauðburður. Then all the sheep are turned loose across the countryside for the summer. Free-range grazing is much cheaper than buying feed and, if a few of them are lost falling off a cliff or being hit by a car (sheep are apparently not very bright), it isn’t a big loss. Lamb is one of the main animal proteins in the Icelandic diet (the other is fish), and most lambs go to slaughter when they are 4-5 months old, undoubtedly disturbing the increasing numbers of vegans in the country.
Smölun, the annual sheep gathering begins in September. Farmers, their families and friends gather to herd the estimated 380,000 sheep intoRéttir, large pens where they are sorted by earmarks, then sent back to the farms for the long, cold Icelandic winter. The roundup concludes with Réttarball, a celebration with live music and considerable amounts of alcohol.
Sightseeing by bus can be rather disappointing. You get off the bus, wander around the site for fifteen to twenty-five minutes, maybe relieve yourself or buy tchotchkes at the requisite gift shop, before being herded back onto the bus like cattle. It seems none of the tourist attraction parking lots are paved; they are covered with pieces of black rock which makes ambulating difficult for those with walker, canes or poor balance. Peg stayed on the bus during many of our subsequent stops.
Seljalandsfoss Seljalandsfoss (pronounced “selya-lands-foss”) is fed by melting water from the nearby Eyjafjallajökull (pronounced “ay·uh·fyaat·laa·yow·kl”) glacier which covers the volcano that erupted in 2010, disrupting air travel in across Northern and Western Europe. The water plunges almost 200 feet to the meadow below. If one is in good physical shape, there is a foot path from the parking lot that winds around the back of the falls, providing a spectacular view and a good soaking. (One foresighted couple brought light rain pants.) I made it part of the way up the hill, took a few pictures and went back to Peg, who was waiting on a bench next to the parking lot.
Seljalandsfoss Waterfall
The stairs leading to the path behind the waterfall
Reynisfjara We continued on to Reynisfjara Black Sand Beach, (pronounced “ray-nis-fyah-ra”) about 36 miles farther east, which lies at the base of Mt. Reynisfjall. Reynisdrangar, large basalt columns, lie just off the beach shore and were used in Game of Thrones Season 7. According to legend, they were formed when two trolls tried to grab a passing ship, but when the sun rose, they turned to stone. Another legend says two different trolls murdered a woman; her husband found them, dragged them into the sunlight and turned them to stone.
One of the offshore basalt columns
The beach can be dangerous. Visitors have lost their lives when large “sneaker” waves, up to 120 feet tall, suddenly appear and pull anyone too close into the ocean. Our guide warned everyone to stay well away from the water’s edge, but predictably some people threw caution to the wind.
Vik Vík í Mýrdal, Vik for short, is a small village 3 miles east of the beach as the crow flies, but 7 miles by road. It lies directly south of the Mýrdalsjökull (pronounced “myir-tals-yo-kʏt”) glacier which covers the Katla volcano, which last erupted in 1918. Residents know they have only 15 minutes to evacuate if there is another eruption, as melting glacier water would quickly obliterate the town.
Mýrdalsjökull
The 2010 Eyjafjallajökull eruption covered Vi kin ash. In 2021 Icelandic director Baltasar Kormákur and writer/producer Sigurjón Kjartansson created KATLA, a mystery-drama television series for Netflix. The plot: a year after Katla erupts, people thought to be dead or missing begin to reappear out of the ash. This creates conflict for the residents who eventually realize they are changelings, not their departed loved ones. I highly recommend checking it out.
Skógafoss Despite the proximity, Vik wasn’t on the itinerary. Instead, we drove back to Skógafoss Waterfall, a thundering spectacle 200 feet high and 82 feet wide. The water’s source, The Skógá River, originates near the Eyjafjallajökull and Mýrdalsjökull glaciers. The hardier and more adventurous can hike the five-mile Skógá Trail to the bridge at the head of the river, AFTER climbing the 527 steep steps to the top of the falls. Spray from the falls creates single or double rainbows when the sun is out.
The long climb to the top of the falls
As with many other sites, Skógafoss comes with its own legend. A Viking settler, Þrasi Þórólfsson, hid a treasure chest behind the falls in 900; the first person to go behind the falls will find riches.
Skogafoss Waterfall
There are three places at the falls for overnight stays: Hótel Skógafoss, Hótel Skógá (both owned by EJ Hotels) and the Guesthouse Skógafoss. Campsites next to the lodging provide an alternative; there’s a parking lot beyond that. A new parking lot was under construction when we were there. The tourism industry has criticized the project, noting the increased distance to the falls (500m or 5.5 football fields) will negatively impact the elderly and disabled.
The parking lot was uneven, and Peg stayed on the bus. I wandered around a bit and took photos of people hiking up and down the stairs to the lookout point.
For some reason, this guy decided to lie down in the wet gravel and take a nap. No, he wasn’t dead.
We boarded the bus, again waiting for the recalcitrant couple, and headed towards Boutique Hotel Anna, midway between Seljalandsfoss and Skogafoss, for a buffet lunch. They put on quite a spread with a delicious salad, beef roast, vegetables, bread and desserts. Sated, watered and rested, we got back on the bus for our final stop.
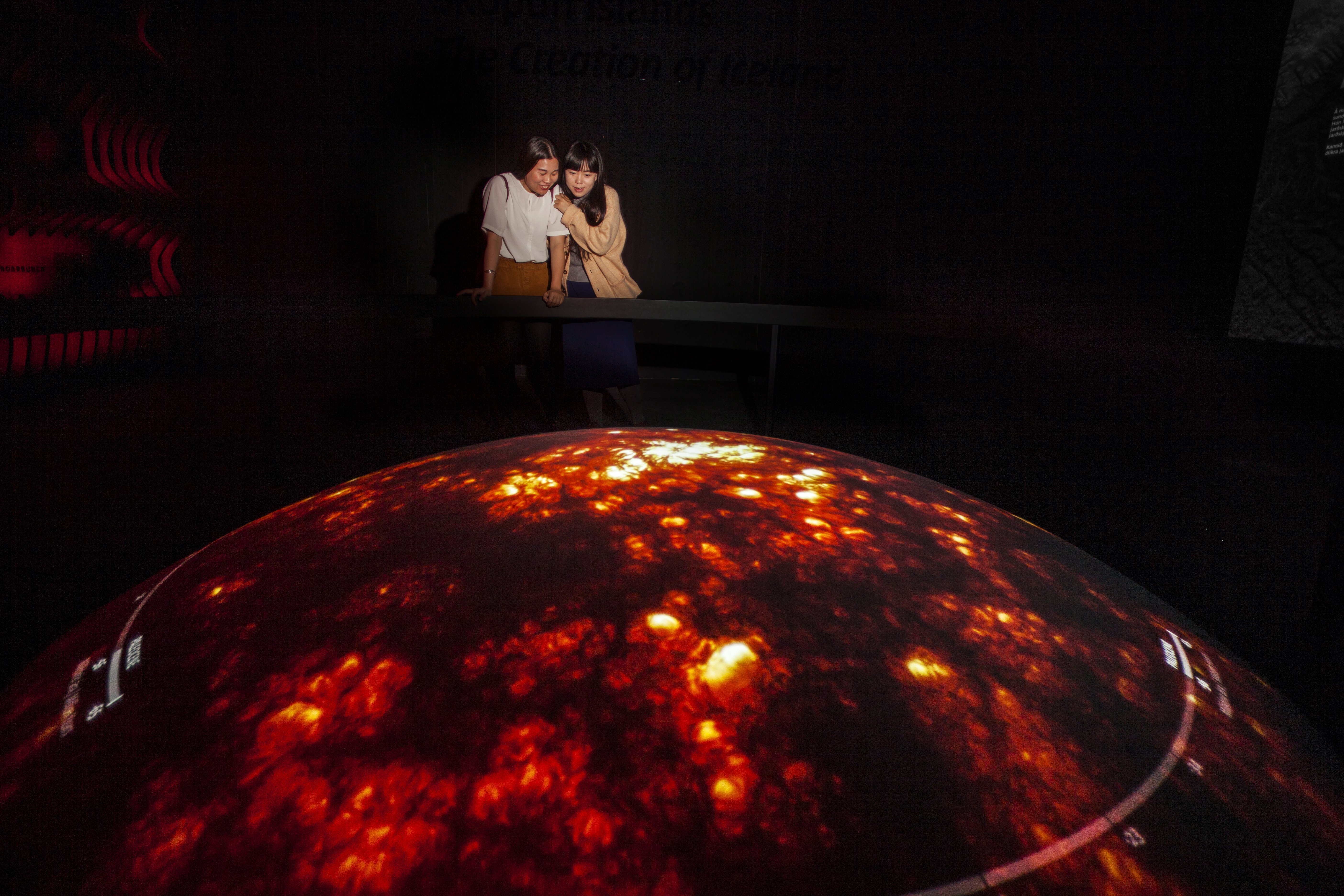
Lava Centre The Lava Centre is in Hvolsvöllur, where we made a pit stop at the beginning of our tour. Our visit started with a 15-minute high-def film of volcanic eruptions around the island. We then gathered around a large map in the reception area while our museum guide explained the geology of the island’s volcanic systems.
From there we walked down a long, dark tunnel chronicling eruptions of years past.
Photographer: Magnus Elvar Jonsson. Used with permission of The Lava Centre
The corridor led to another room where we learned about the earth’s evolution. The handrail around the display moves the image through time, from the hot ball of rock 4.5 billion years ago, through the shifting tectonic plates and island’s geography to the present.
Photographer: Magnus Elvar Jonsson. Used with permission of The Lava CentreUsed with permission of The Lava Centre
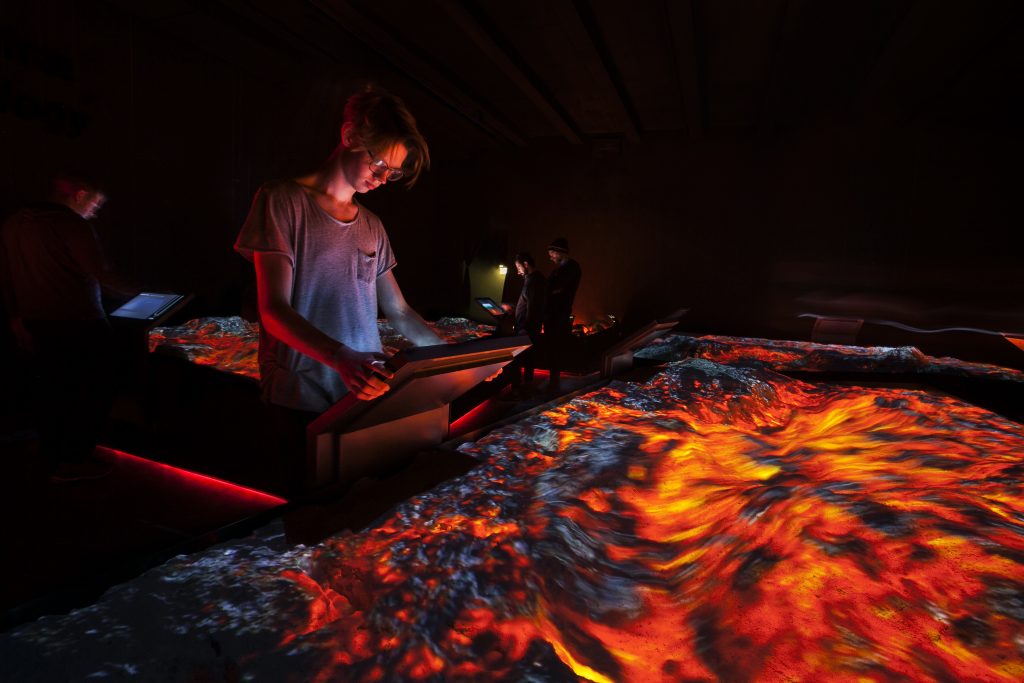
We then continued through another short passage where one can experience an earthquake by standing on a concrete pad which vibrates violently, accompanied by an ear-splitting explosion. The exhibit ends in a room with a simulated mantle plume and lava flows.
Lava Plume. Used with permission of the Lava CentrePhotographer: Magnus Elvar Jonsson. Used with permission of The Lava Centre
The trip back was an hour and a half; at one point the fog was so thick we wondered if the driver could see the road.
Finally, we were back at the port; we boarded the ship and headed to our stateroom for a short rest.
We went to the World Café for dinner at 6pm, but it was a feeding frenzy of old people who appeared not to have been fed for days. So, we took the elevator down to The Living Room. There’s a bar that serves soft drinks and cocktails, charged to one’s room, but coffee, tea and pastries are available for free. We had drinks and relaxed on comfortable chairs while a piano and flute duo performed classical pieces.
World Café The World Café is a large, horseshoe-shaped venue on Deck 7, in the aft third of the ship just across from the elevators. Tables for two to six or more sit on the perimeter; the expansive floor-to-ceiling windows provide light and views of the sea. Each side starts with a drink station where one can get juice, water and ice; the coffee machine dispenses hot water for tea, hot chocolate and creates espresso/cappuccino, adding foamed or steamed milk automatically from an adjacent dispenser.
Food is served from buffets in the middle of the Café, starting with appetizers, moving on to main courses, and ending with a bread/dessert bar. One side usually has pizza slices. There’s a specialty station along the back where one could get more exotic noodle dishes (Asian and Italian). A full-service bar across with bar stools and tables faces the specialty station. The kitchens are in the interior of the food service areas. Doors on either side of the bar open onto the Aquavit Terrace for outside dining. Guests can also take a dip in the hot tub and infinity pool.
The waitstaff brought water to our table and took orders for soft drinks, wine, beer or cocktails. I usually started with sashimi – raw salmon or scallops with pickled ginger and wasabi. Peg opted for a salad or some soup. The entrées changed every day but usually featured lamb and fish with a variety of sides. We were impressed by the hefty sneeze guards over the food, and by the entrée descriptions which listed potential allergens (nuts, wheat, milk, egg).
Dessert choices included a variety of small (one or two bite) cakes, brownies, cups of mousse and a nice selection of ice cream and gelatos. Peg often had tea with dessert and I would get a cappuccino from the self-service machine.
The ship left port as we finished our dinner, headed for our first stop on the cruise. Our tired bodies sank into the soft bed and sleep, again, came quickly.
Next: Day 3 – Isafjödur and Bolungarvik. Trolls and tunnels, a troubadour and a fisherman, and another waterfall.
Arriving in Reykjavik a day ahead to recuperate was a very good idea. Going from the airport directly to the ship would have left us more exhausted than we already were.
The Skarfabakki Harbor Cruise Terminal is about three miles from the hotel, and a much cheaper cab ride. We were fortunate that our ship, the Viking Mars, docks at Skarfabakki 315. Other ships dock down the street at Skarfabakki 312, a long hike from our drop-off point The old terminal was demolished to make way for a new terminal scheduled to open in 2026..
The ship’s crew took our luggage after the cab dropped us off; Viking has set up a temporary facility that made boarding (“embarkation” if you want to be formal) efficient and easy. We entered this building, showed our passports and boarding passes, and walked outside to the boarding ramp. High tide made for a steep climb, but one of the crew took Peg’s Rollator ahead while she grabbed the railing.
Viking Mars embarkation building
Once inside the ship, the staff scanned our boarding passes, which put us into their system, gave us our room keycards, and offered us a hot, wet washcloth and glass of champagne. Then, they directed us down the hallway to The Restaurant where another crew member went through the mandatory safety evacuation protocol: how to put on the life vest and where to go if needed.
(At this point, I recommend getting a lanyard for your keycard. Otherwise, you’ll be fishing in your wallet or purse for the damned thing and risk losing it, as I did.)
We had to wait until 1p.m. before we could get into our rooms, so we went up to the World Café, a self-service buffet, on Deck 7 for a bite to eat.
After lunch we made our way to our stateroom, a long walk almost to the end of the narrow hallway. Our cabin steward, a friendly Indonesian man, greeted us by name. “Dr. Rivera and Mrs. Sullivan.” (All future greetings were an enthusiastic “Dr. David and Mrs. Mary!”) Our suitcases sat outside our stateroom door. He pushed them into the room and then hefted one of them onto the large vinyl pad covering the foot of the bed to protect the bedding while unpacking before orienting us to our room.
My fat ass in the doorway of our stateroom
The large sliding glass door at the end of the room opens onto a veranda with two chairs and a small table. An armchair sits just inside. There’s a couch to the right of the chair; a large wooden tray with Viking brochures and a copy of The Viking Daily – with a synopsis of the port stop, a morning-to-evening list of the day’s onboard activities, departure times for shore excursions, the dining hours, and a ship services directory with phone numbers – sits on a coffee table in front of the couch.
The long desk has drawers for storage at the near end and a mini fridge at the far end stocked with Sprite, regular Coke and Coke Zero; Carlsberg beer; tonic water; travel bottles of Bacardi Rum, Beefeater Gin, Smirnoff Vodka, and The Famous Grouse Scotch; two small milk chocolate bars, and two bags of nuts, all replenished once a day. (Our steward switched out the regular coke for Coke Zero after Peg left him a note saying we didn’t drink sugared pop.) We had a complementary bottle of champagne and two flutes waiting for the right time to celebrate.
The middle of the desk opens up to a lighted mirror, a pair of binoculars and abundant storage for cosmetics and toiletries. The devices next to the hair dryer are QuietVox audio receivers used for self-guided tours or for one’s tour director to herd the cattle back to the bus.
The king-sized bed has four pillows (Peg asked and received an extra), a comforter, sans top sheet, and a “Traditional Norwegian Marius-weave blanket.” Each side has a night stand with 110/220V outlets, two USB charging ports and a wall lamps. The switch just above the electrical bar turns on the nightlight for bathroom trips. The two little silver circles are reading lamps.
A credenza with even more drawers and two shelves sits across from the bed. The ship supplies a large carafe of water and two lovely blue drinking glasses, along with a card that said, “if you like these items, they are available for purchase.” Subtext, “if you steal these glasses, we’re gonna add $200 to your tab!”
A 42” television is mounted on the wall above. There are several programming options: movies, TV series, news channels (Fox, CNN, BBC), a variety of music choices whose categorization left much to be desired, broadcasts of previous lectures (which is how I found out Bluetooth was named after Harald Bluetooth, a 10th century Danish and Norwegian king), and the perpetual view from the bridge camera, overlaid with classical music. My Cousin Vinny was one of the movie selections; however, we didn’t think showing Lifeboat and Titanic on a cruise ship was a wise choice.
Bow camera view of Isafjödur’s port
The bathroom was superb! It has a heated floor which is so efficient I had to turn it off because the temperature became stifling. There are drawers on each side of the sink and toiletry racks for Viking’s “Premium Freyja® toiletries” on either side of the anti-fog mirror. We found large, fluffy towels and washcloths under the counter.
The wall-mounted toilet is very efficient and very loud when flushed. I’d like these in my retirement house because cleaning the bottom of a floor-mounted toilet is a colossal pain.
The shower is more than adequate despite appearing rather narrow in this picture. The knob on the left turns the water on; the one on the right controls the temperature. I discovered a button on the back that overrides the water temperature limiter if one wants hotter water. The water flow decreases if one opens the shower door while the water is running. I should note that showering while the ship is sailing requires some caution. Peg only showered when the ship was in port to avoid being hurled out the shower door in rough seas.
There’s abundant closet space opposite the bathroom with a lot of wooden hangers on one side and more than sufficient drawer space on the other, hidden by sliding doors with magnetic catches. There are two decent sized robes on hangers, and a wooden box on the floor holds two pairs of complementary slippers (I could only get half of my foot into one) and a bright red Viking umbrella for rainy shore excursions.
A shelving unit next to the closet houses a Nespresso coffeemaker, a safe behind a cabinet door, and more drawers, one of which housed a horse hair lint brush, a shoe shine brush and instructions for complementary clothes pressing, returned the next day.
After unpacking, putting drawer things in drawers and hanging things on hangers, it was time for another nap. We woke up around 5:30pm and arrived at The Chef’s Table just before it opened for dinner.
There was a line of people waiting at the restaurant desk to make reservations for the ship’s two specialty restaurants: The Chef’s Table and Manfredi’s Italian Restaurant., (Our booking class had allowed us to make reservations 70 days before the cruise departed, so we were all set.) Our host took us to a table in a bright corner near the back, next to the windows.
Beauty and her beast
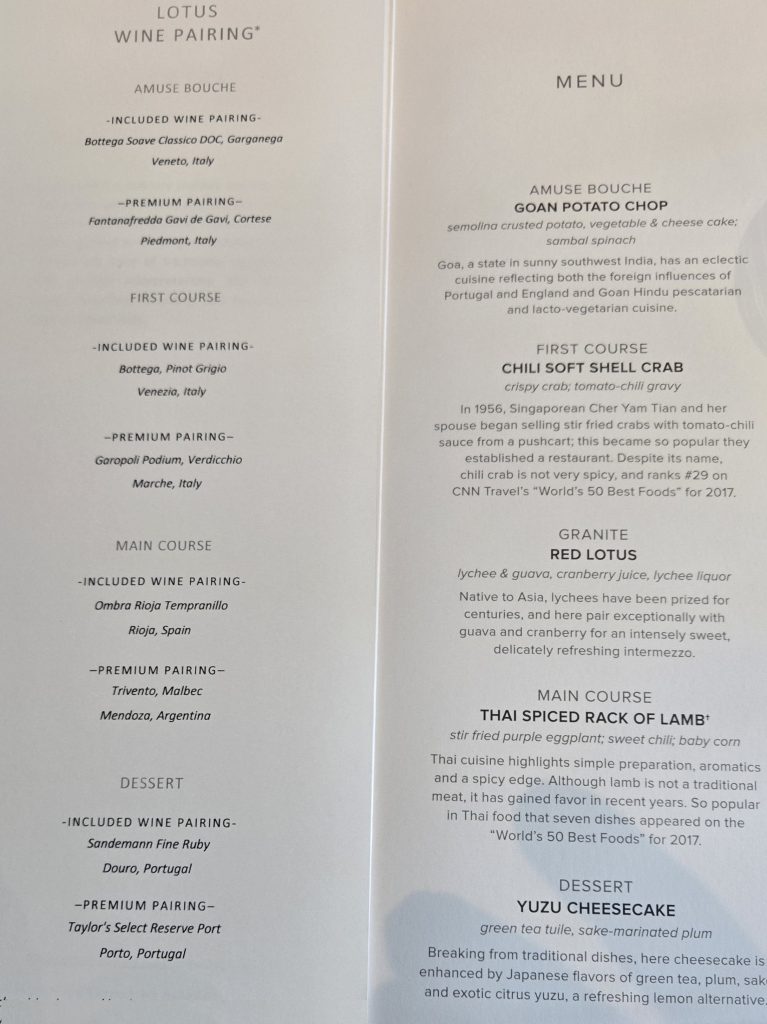
Our four-course menu started with the “Amuse Bouche,” a fancy name for appetizer that conjures an image of Beavis saying, “funny bunghole.” The Goan Potato Chop was a light vegetable and cheese stuffed croquette, served with Soave Classico, an Italian white wine. The first course was Chili Soft-Shell Crab in a light tomato-chili sauce, paired with a nice glass of Pinot Grigio another Italian white. (You can probably guess where this is headed.)
I’m not into food porn; I started taking pictures when our palate cleanser, a lychee, guava and cranberry juice granite named Red Lotus arrived.
Our main course was Thai Spiced Rack of Lamb with eggplant, sweet chili and my sister-in-law’s nemesis, the dreaded baby corn, served with a ruby-red Rioja Tempranillo.
Dessert was a delightful Yuzu Cheesecake, whose namesake fruit provides a lemon flavor, along with fine ruby port.
An amateur restaurant critic seated with a foursome just behind us weighed in on the main course. I thought he might be a Texan, but he mentioned being from Oklahoma in passing. “Well, the lamb was very good but I’m kind of a meat and potatoes and beer guy.” Icelandic animal protein sources are largely lamb and fish, although beef would be available on the cruise.
He and his wife were celebrating their 40th anniversary; the waitstaff presented them with a chocolate ganache-covered mousse, the size of a small curling stone, along with a glass of champagne. The couple at the table next to us were celebrating their 50th anniversary and must have married young, because they didn’t appear to be terribly old; their mousse and champagne arrived shortly after.
Not to be left out, our waiter brought us a berry mousse covered with a strawberry ganache. And a glass of champagne. By this time my photographic skills were sorely lacking.
Fully sated and slightly toasted from the wine we had with dinner, we headed back to our room for bed. Our waiter graciously offered to send the leftover mousse to our room for us to enjoy over the next couple of days.
There’s no chocolate on the bed with the turndown service, but neither did we find the whimsical towel creations on the bed which are popular with other cruise lines that seem intent on forcing your happiness. I hung the room service request for breakfast outside door and sank into our nice soft bed. The Southern Coast of Iceland bus tour started 7:30am, an ungodly hour to be doing anything.
The best thing about dinner? Peg didn’t need time to “wind down” while fighting sleep. A few minutes under the covers and she was out.
Next: Touring the Southern Coast of Iceland by bus. Geothermal power plants, black sand beaches, waterfalls everywhere and a stop at the Lava Centre.
When you have the time, you won’t have the money. When you have the money, you won’t have the time. When you have the time and the money, you won’t have the energy.
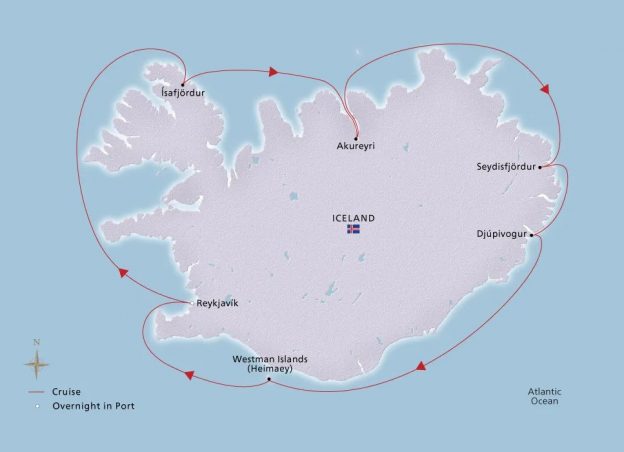
I’ve been wanting to go to Iceland since my 50th and 60th birthdays. We decided to combine my 70th with our 25th wedding anniversary and take a cruise around the island. Better late than never
We left from O’Hare’s international terminal, whose recent $1.3 billion expansion just made for a longer walk. We got a quick bite at Rick Bayless’ (famous Chicago chef) Tortas Frontera before heading for a two-hour wait at the gate.
Our flight left Chicago at 10:15pm on Icelandair, albeit on a dreaded Boeing 737 Max. (We survived!) If you’re old and going to do a long flight, I highly recommend shucking out the extra money for business class; it is a very long, six-hour flight. The seats are comfortable and accommodated my fat ass nicely. Each seat had a pillow, a comfy blanket and a cute little welcome bag made of reinforced biodegradable paper with socks, a sleep mask, toothbrush, hand cream and other stuff.
The flight attendants were a hoot; a skinny Indonesian looking guy, wearing an ascot and apparently enamored with his style, and an equally skinny young Nordic man. They treat passengers like royalty. They offered us bottled water, caramel corn, and free headphones (main cabin passengers had to rent them) and menus.
The food was great; delicate portions served on real china plates with real silverware. I tried 64° Reykjavik Distillery’s Angelica Gin, which tasted more like paint thinner and less like the typical juniper-based gin. However, on the way back I discovered their Rhubarb Gin. Very tasty!
The LED screens in the seatbacks provided a map of the jet’s progress along with information on altitude (36,000ft.), cruising speed (600 mph), outside temperature (around -56°F) and departure/destination times. Entertainment options included movies, TV, and Icelandic classical music selections. Peg watched the Barbie movie. I tried sampling the Icelandic music in between glancing at her screen and the one the next row up who was watching The Hitman’s Bodyguard.
About two hours after takeoff, the horizon started to lighten somewhere over Eastern Quebec. The sun was up by the time we reached the middle of the Labrador Sea. We passed over Greenland, but the clouds made it impossible to see the terrain. Finally, we landed in Keflavik at 9:30am local time, a beautiful sunny day. That was the last time we’d see the sun for the rest of the trip.
Getting off the plane provided our first shock. Tourist traffic has completely overwhelmed Keflavik International Airport and the crowds are worse than O’Hare. We had to walk down aluminum stairs rolled up to the aircraft; only departing flights get a jet bridge. The Rollator we gate-checked at O’Hare and assumed would be at the plane was nowhere to be found; we figured it went to baggage claim. We hobbled over to the buses that took us to the South Terminal, where we funneled in through a single set of doors like cattle being led to the slaughter.
Once inside, we took escalators to the second floor and made the long walk to Customs, entering the maze until the crowd stopped. We saw several Automated Passport Control kiosks wrapped in plastic that might have made the process faster but they hadn’t been installed .We stood in line for about 20 minutes. We finally made it through and took a short break; Peg’s foot was killing her by this time.
There are no people movers in the very long corridor connecting the South Terminal to the Main Terminal. I ran ahead of Peg to find the Rollator, but there was no way to retrieve it and then re-enter the secure area, so I came back, and we just kept walking.
Aerial view of Keflavik Airport
Baggage claim is one floor down; Peg and I took the elevator. The first thing we saw before we got there were the requisite shops, including two familiar American shops:
I picked up our suitcases, but I couldn’t find the oversized luggage carousel, so I asked the young woman at customer service. I followed her (it was in plain sight) and apologized for being so clueless. She said, “That’s all right. You just wanted to meet me.” In the meantime, Peg got cash from a nearby ATM; banknotes come in 500, 1000, 2000, 5000, and 10000 krónur and like most foreign currency, they are very colorful. If that seems like a lot of money, keep in mind 1000 ISK is around $7.25, more or less.
Customs authorities must be very trusting because there were no officials at the “nothing to declare” aisle, so we walked through and found ourselves in the main terminal near the exits, across from the currency exchange Peg had expected near baggage claim. I looked for a bathroom but the nearest facilities were down one floor in a rather secluded area.
We stepped outside to the taxi stands. We could get to downtown Reykjavik for about $68 each via Flybus Airport Transfer, but a friend of Peg’s who has been to Iceland told her it would let us off at a designated bus stop a few blocks from the hotel. We weren’t going to schlep two suitcases, a Rollator, and a carry-on bag so we opted for a cab.
The nice young man staffing the taxi stand told us there were fewer cabs than usual, which at that time meant none, except for an empty van with no visible driver. They arrived one at a time, several minutes apart. We stood in line with a few other passengers and enjoyed our first view of Iceland on the ground.
Predictably, there was one American asshole who pushed to the head of the line, thinking he should take priority. He wanted to go to the Parliament Hotel in Reykjavik and tried to bum a ride with a couple that was going into Keflavik. The next available cab was a full-sized SUV. Peg asked the driver, “Is the Hotel Konsulat near the Parliament?” The asshole quickly interjected, “No!” Seriously? Later Google maps indicated the two hotels are about 4 blocks apart. It’s probably better that we didn’t ride with him.
Downtown Reykjavik is about 31 miles from the airport. The landscape between Keflavik and Reykjavik looks like Eastern Montana; very rough terrain covered with moss, the first thing to grow on volcanic rock. The highways are two-lane and not as wide as our Interstate or major US highways. They were well maintained, without the abundant and often perpetual potholes in the Midwest.
Highway outside Keflavik
We approached the outskirts of Reykjavik and, while most of the businesses have Icelandic names, signs on the buildings have a mixture of English and Icelandic. And Iceland isn’t immune from American influences; we saw Subway, Domino’s Pizza and KFC. There are no Starbucks in Iceland because, as this What’s On article notes:
“The absence of Starbucks in Iceland is not a sign of a lack of coffee culture; rather, it represents a conscious choice to prioritize local businesses and foster a thriving scene for specialty coffee. Icelanders value the craftsmanship and dedication of their local roasters and baristas, who treat coffee with the same reverence that they extend to their beloved natural landscapes.”
Gasoline in Iceland is expensive, about $9.60 a gallon when we were there. Most of the cars we saw were small, including an electric Nissan Leaf, but there were a few Beemers and Mercedes. The Orkan petrol chain, with its bright pink color scheme, advertises “Cheap Gas.” N1 and Olís stations tend to be more expensive
Our driver took us through narrow streets in the downtown area before stopping in front of the Reykjavik Konsulat Hotel, which one would miss it if walking by casually. There is no big lighted sign and no parking lot, and the door isn’t automatic. That is because it was formerly a department store in the early 1900s, owned by Konsul Ditlev Thomson.
The hotel is very charming. The reception area and the wine room off to the left are done in dark wood. The elevators are very narrow; one of them could only hold two people. The top part of the car is papered with old photos of a store or apothecary shop; the bottom was wood, looking like rows of small drawer fronts. You can see more photos of the hotel at their Facebook page.
Our room was on the 4th floor, small by American standards, but typical of European hotel rooms and quite cozy. The first thing we noticed was the king-sized bed had two individual comforters and no top sheet! The bathroom walls had large tiles from floor to ceiling; the wall behind the sink was done in mosaic tile. The shower had two heads, and the body wash, shampoo and conditioner were in refillable bottles.
There was a very small balcony through a narrow door just to the right of our bed. I took these pictures of the Radisson Blu 1919.
Eimskip is an Icelandic shipping company. (According to Google Translate eimskip is “steamship”, and eimski is “stupid.” What a difference a letter makes.)
We were exhausted. Bu this time it was noon local time and we’d been up for 24 hours, so we got comfortable and jumped into bed for what turned into a five-hour nap. Neither one of us had the energy to find a restaurant after we got up, so we went downstairs to the bar to the right of the reception desk. It was quiet and cozy, with floor to ceiling windows, comfortable chairs and an attentive bartender. Peg ordered Iceland’s domestic beer, Gull, and I had a glass of white wine. Prohibition in Iceland began in 1915 and, while wine and spirits were legalized in 1922 and 1935, respectively, beer only became legal in 1989.
Bæjarins Beztu Pylsur (The Town’s Best Sausages), sitting just outside the bar, is the iconic hot dog stand that’s been in downtown Reykjavik since 1937. Icelandic hotdogs, made with lamb, are longer than our domestic dogs, and can be customized with Remolaði sauce, Icelandic mustard, fried or raw onions, and a ketchup sweetened with apples instead of sugar. They are also relatively cheap, about ISK790, or a little less than six bucks. There are people lined up in all seasons, but they are served quickly. We noticed two things: everyone paid with a credit card and the soft drinks are small; no extra-large or Big Gulps. The straws are recyclable; Iceland banned single-use plastic in 2021. You can see the crowd over Peg’s shoulder.
There is no real night in Iceland during the weeks either side of the summer solstice, only a four-hour period of dusk. The downside is there’s only a four-hour period of daylight during the weeks around the winter solstice.
Reykjavik, 12pm, July 26, 2024Reykjavik, 12am July 27, 2024
I opened the balcony door in the middle of the night; there isn’t any air conditioning, and the room was becoming stuffy. There’s a bar, Hornið (trans: the corner), on the street and the rowdies sitting outside were at it until at least 3am. Someone was singing, “I don’t wanna wait,” but my sleep-deprived brain kept hearing “Power 108” as in “KPWR 108.3 FM.” (Actually, KPWR is a real radio station in Los Angeles, “Power 106” – 105.9FM)
We slept in and missed the hotel’s breakfast buffet, so Peg had hot tea while we waited for the 11 am cab we had arranged. I considered going across the street to Joe & The Juice for a cappuccino, but I didn’t want to miss our ride. (I discovered Joe & The Juice isn’t exclusive to Iceland; there are stores across Europe and seven in Chicago!)
I regret we were about to leave Reykjavik without having visited Hið Íslenzka Reðasafn, The Icelandic Phallological Museum. Maybe next time.
Next: Embarkation (fancy talk for boarding the ship)
Aerial view of Keflavik Airport. (C) 2017 by Eric Salard. Licensed under Creative Commons CC BY-SA 4.0